




 |
 |
| J Korean Med Assoc > Volume 53(1); 2010 > Article |
Abstract
Osteoporotic vertebral fractures suspected at clinical evaluation require radiological confirmation. Most radiologists make the diagnosis of vertebral fracture on the basis of a qualitative impression. However, unlike other fractures, vertebral fractures are commonly found on radiographs obtained for other reasons in patients who do not show signs or symptoms suggestive of fractures. Radiologists qualitatively analyze radiographs of the thoracolumbar spine to identify vertebral fractures in patients whose clinical indications suggest trauma, osteoporosis, malignancy, or acute back pain. The accuracy of decision-making process can be enhanced by additional radiographic projections or by complementary examinations including DXA (Dual Energy X-ray Absorptiometry) morphometry, bone scan, CT, or MRI. The importance of imaging is highlighted by the fact that only about one in four vertebral fractures is recognized on the basis of clinical evaluations without radiographs. Radiographs may include lateral and AP (anterior/posterior) X-rays of the affected spinal segments. The physician may request bone scan and/or CT to help identify the location of the fracture, its status (stable versus unstable). Furthermore, an MRI scan may be performed if neurologic deficit, soft tissue trauma or hematoma are suspected.
References
1. Saville PD. A quantitative approach to simple radiographic diagnosis of osteoporosis: Its application to the osteoporosis of rheumatoid arthritis. Arthritis Rheum 1967;10:416-422.
2. Rogers LF, Lenchik L. In: Juhl JH, Crummy AB, Kuhlman JE, editor. Metabolic, endocrine, and related bone disease. Essentials of radiologic imaging 1998;7th ed. Lippincot-Raven. 199-236.
3. Yang SO, Choi MY. Diagnositic imaging features of osteoporosis. Korean J Osteoporosis 2004;2:1-8.
4. Cook GJ, Hannaford E, See M, Clarke SE, Fogelman I. The value of bone scintigraphy in the evaluation of osteoporotic patients with back pain. Scand J Rheumatol 2002;31:245-248.
5. Schousboe JT, DeBold CR, Bowles C, Glickstein S, Rubino RK. Prevalence of vertebral compression fracture deformity by X-ray absorptiometry of lateral thoracic and lumbar spines in a population referred for bone densitometry. J Clin Densitom 2002;5:239-248.
6. Mayo-Smith W, Rosenthal DI. Radiographic appearance of osteopenia. Radiol Clin North Am 1991;29:37-47.
7. Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Mineral Res 1993;8:1137-1148.
8. Yang SO. Clinical use of dual-energy X-ray absorptiometry. Korean J Bone Metab 1996;3:128-135.
9. Schousboe JT, Vokes T, Broy SB, Ferrar L, McKiernan F, Roux C, Binkly N. Vertebral fracture assessment: The ISCD official positions. J Clin Densitom 2008;11:92-108.
10. Haller J, André MP, Resnick D, Miller C, Howard BA, Mitchell MJ, Schils JP, Sartoris DJ, Trudell D. Detection of thoracolumbar vertebral body destruction with lateral spine radiography. Part II. Clinical investigation with computed tomography. Invest Radiol 1990;25:523-532.
11. Kim JI, Yang SO, Choi JC. MRI findings of vertebral compression fractures. J Korean Radiol Soc 1995;33:667-672.
12. Cuénod CA, Laredo JD, Chevret S, Hamze B, Naouri JF, Chapaux X, Bondeville JM, Tubiana JM. Acute vertebral collapse due to osteoporosis or malignancy: appearance on unenhanced and gadolinium-enhanced MR images. Radiology 1996;199:541-459.
13. Baur A, Stabler A, Arbogast S, Duerr HR, Bartl R, Reiser M. Acute osteoporotic and neoplastic vertebral compression fractures: fluid sign at MR imaging. Radiology 2002;225:730-735.
14. Yamato M, Nishimura G, Kuramochi E, Saiki N, Fujioka M. MR appearance at different ages of osteoporotic compression fracture of the vertebrae. Radiat Med 1998;16:329-334.
15. Kong JH, Park JS, Ryu KN. Osteoporotic compression fracture of the thoracolumbar spine and sacral insufficiency fracture: incidence and analysis of the relationship according to the clinical factors. J Korean Radiol Soc 2006;55:495-500.
16. McAfee JG. Radionuclide imaging in metabolic and systemic skeletal disease. Semin Nucl Med 1987;17:334-349.
17. Karchevsky M, Babb JS, Schweitzer ME. Can diffusion-weighted imaging be used to differentiate benign from pathologic fractures? A meta-analysis Skeletal Radiol 2008;37:791-795.
18. Favus MJ. Primer on the metabolic bone diseases and disorders of mineral metabolism 1996;3rd ed. Philadelphia: Lippincott-Raven. 152-163.
19. Dass B, Puet TA, Watanakunakorn C. Tuberculosis of the spine (Pott's disease) presenting as 'compression fractures'. Spinal Cord 2002;40:604-608.
20. Korean Soc of Bone and Mineral Metabolism. Osteoporosis 2006;Hanmi Publishing Company. 134-147.
21. Kalpakcioglu BB, Morshed S, Engelke K, Genant HK. Advanced imaging of bone macrostructure and microstructure in bone fragility and fracture repair. J Bone Joint Surg Am 2008;90:68-78.
Figure 2
Various type of vertebral compression fractures: From left, wedge type, biconcave type, and pancake-like crushed vertebral fracture.
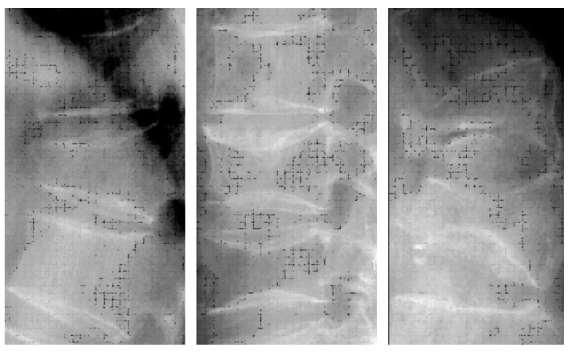
Figure 3
Semiquantitative method to assess vertebral fractures. (Genant HK, et al. J Bone Mineral Res 1993; 8(9):1137-1148).
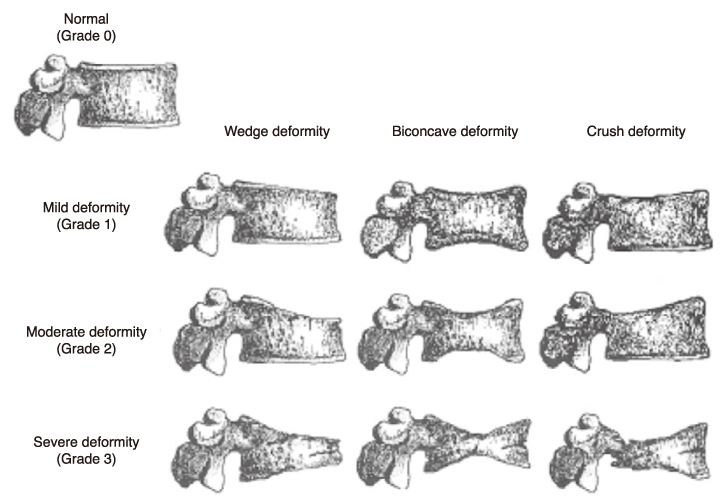
Figure 5
Compression fracture of the 1st lumbar vertebral body by bone scan (left) and sacral insufficiency fracture by bone SPECT (right).
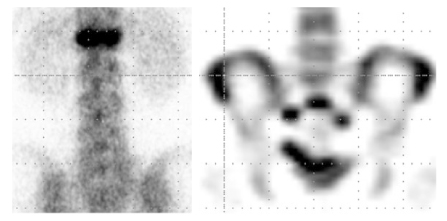
Figure 6
CT sagittal reconstructed image and 3 D reformation of L2 vertebral fracture in 62 year-old male.
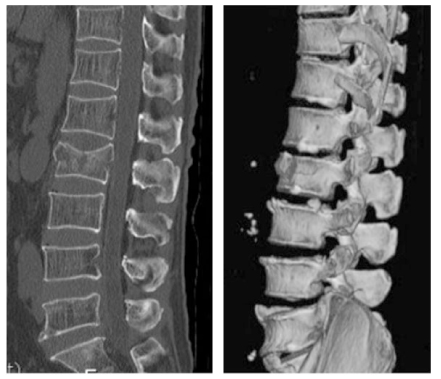
Figure 7
MRI finding of benign vertebral fracture: T2 WI, T1 WI, T1 contrast enhanced image (from left).

Figure 8
MRI finding of malignant vertebral fracture: T2 WI, T1 WI, T1 contrast enhanced image (from left). Note the exophytic soft tissue mass and signal changes in the whole spine.
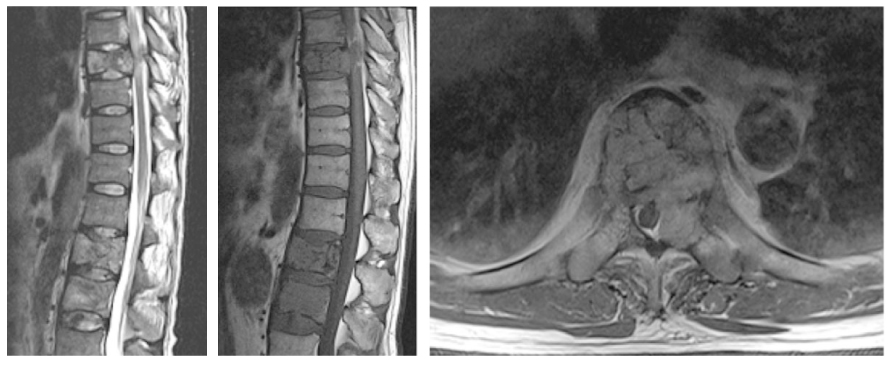
Figure 9
MRI finding of sacral insufficiency fracture: Fat suppressed sagittal T2 WI, axial T1 WI, axial fat suppressed T1 WI (from left).
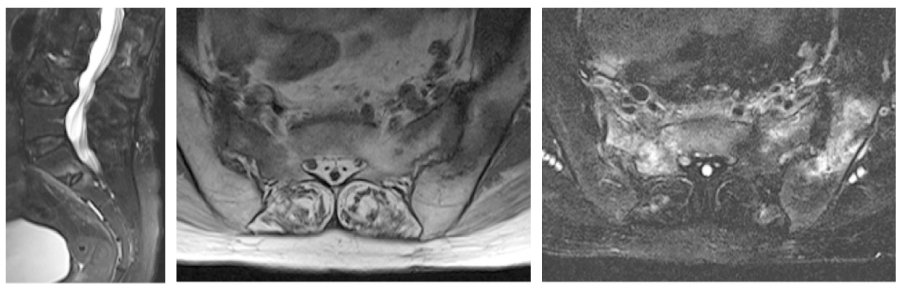
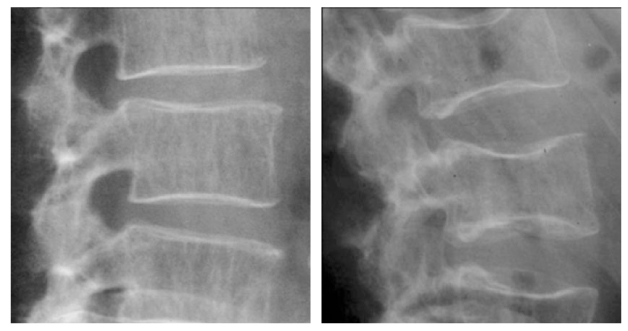
Figure 10
Simple radiographs of two cases with multiple myeloma: Heterogenous osteolytic bone loss and biconcave fractures.
- TOOLS
-
- Share :
-





- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
