



 |
 |
| J Korean Med Assoc > Volume 51(10); 2008 > Article |
Abstract
Sexually transmitted diseases (STDs) are not rare during pregnancy; however, they are usually asymptomatic and may be unrecognized. STDs in pregnancy can cause serious complications to both pregnant women and fetuses. Screening tests are recommended, because the treatment of these diseases can be curative in most cases, or at least effective in reducing complications. In this point of view, the Centers for Disease Control and Prevention recommends screening of all pregnant women for several STDs including human immunodeficiency virus (HIV) infection, hepatitis B, and syphilis, and screening selectively in high risk women for gonorrhea and hepatitis C. To reduce vertical transmissions, highly active antiretroviral therapy and timed Cesarean delivery is recommended in HIV-infected pregnant women. Penicillin is still a drug of choice for syphilis in pregnancy. In women who have active genital herpetic lesions at the time of labor, Cesarean delivery is indicated to protect neonates from perinatal transmissions. However, in women who have genital warts with human papilloma virus infection, Cesarean delivery is not recommended to prevent neonatal laryngeal papillomatosis. In women infected with gonorrhea, Chlamydia or Trichomonas, tests for HIV infection are recommended because of high prevalence of concomitant infections.
References
1. Donders GG, Desmyter J, De Wet DH, Van Assche FA. The association of gonorrhoea and syphilis with premature birth and low birthweight. Genitourin Med 1993;69:98-101.
2. Majeroni BA, Ukkadam S. Screening and treatment for sexually transmitted infections in pregnancy. Am Fam Physician 2007;76:265-270.
3. Golden MR, Marra CM, Holmes KK. Update on syphilis: resurgence of an old problem. JAMA 2003;290:1510-1514.
4. Nathan L, Bohman VR, Sanchez PJ, Leos NK, Twickler DM, Wendel GD Jr. In utero infection with Treponema pallidum in early pregnancy. Prenat Diagn 1997;17:119-123.
5. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep 2006;55:1-94. Erratum in: MMWR Recomm Rep. 2006; 55: 997.
6. Wendel GD Jr, Sheffield JS, Hollier LM, Hill JB, Ramsey PS, Sánchez PJ. Treatment of syphilis in pregnancy and prevention of congenital syphilis. Clin Infect Dis 2002;35:S2. S200-S209.
7. Klein VR, Cox SM, Mitchell MD, Wendel GD Jr. The Jarisch-Herxheimer reaction complicating syphilotherapy in pregnancy. Obstet Gynecol 1990;75(3 Pt 1):375-380.
8. Augenbraun MH. Treatment of syphilis 2001: nonpregnant adults. Clin Infect Dis 2002;35:S2. S187-S190.
9. Christmas JT, Wendel GD, Bawdon RE, Farris R, Cartwright G, Little BB. Concomitant infection with Neisseria gonorrhoeae and Chlamydia trachomatis in pregnancy. Obstet Gynecol 1989;74(3 Pt 1):295-298.
10. Andrews WW, Klebanoff MA, Thom EA, Hauth JC, Carey JC, Meis PJ, Caritis SN, Leveno KJ, Wapner RJ, Varner MW, Iams JD, Moawad A, Miodovnik M, Sibai B, Dombrowski M, Langer O, O'Sullivan MJ. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Midpregnancy genitourinary tract infection with Chlamydia trachomatis: association with subsequent preterm delivery in women with bacterial vaginosis and Trichomonas vaginalis. Am J Obstet Gynecol 2006;194:493-500.
11. American Academy of Pediatrics and American College of Obstetricians and Gynecologists. Guidelines for Perinatal Care 2002;5th ed. Washington, DC: AAP and ACOG.
12. Donders GG. Management of genital infections in pregnant women. Curr Opin Infect Dis 2006;19:55-61.
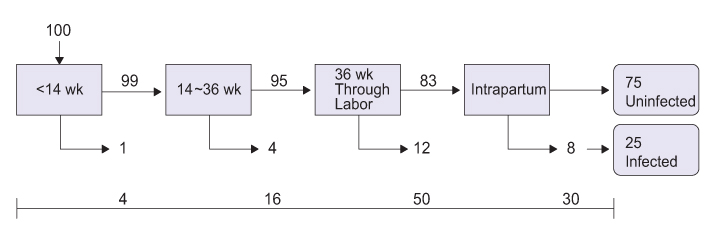
13. Harger JH, Amortegui AJ, Meyer MP, Pazin GJ. Characteristics of recurrent genital herpes simplex infections in pregnant women. Obstet Gynecol 1989;73(3 Pt 1):367-372.
14. Nahmias AJ, Josey WE, Naib ZM, Freeman MG, Fernandez RJ, Wheeler JH. Perinatal risk associated with maternal genital herpes simplex virus infection. Am J Obstet Gynecol 1971;110:825-837.
15. ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. No. 82 June 2007. Management of herpes in pregnancy. Obstet Gynecol 2007;109:1489-1498.
16. Clinton WJ. Turning the tide on the AIDS pandemic. N Engl J Med 2003;348:1800-1802.
17. Centers for Disease Control and Prevention. Achieve-ments in public health. Reduction in perinatal transmission of HIV infection-United States, 1985-2005. MMWR Morb Mortal Wkly Rep 2006;55:592-597.
18. Kourtis AP, Bulterys M, Nesheim SR, Lee FK. Understanding the timing of HIV transmission from mother to infant. JAMA 2001;285:709-712.
19. Cooper ER, Charurat M, Mofenson L, Hanson IC, Pitt J, Diaz C, Hayani K, Handelsman E, Smeriglio V, Hoff R, Blattner W. Women and Infants' Transmission Study Group. Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr 2002;29:484-494.
20. Bulterys M, Jamieson DJ, O'Sullivan MJ, Cohen MH, Maupin R, Nesheim S, Webber MP, Van Dyke R, Wiener J, Branson BM. Mother-Infant Rapid Intervention At Delivery (MIRIAD) Study Group. Rapid HIV-1 testing during labor: a multicenter study. JAMA 2004;292:219-223.
21. U.S. Public Health Service Task Force Perinatal HIV Guidelines Working Group. Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV-1 transmission in the United States 2003;11. 26. March 2004.
http://AIDSinfo.nih.gov
22. The International Perinatal HIV Group. The mode of delivery and the risk of vertical transmission of human immunodeficiency virus type 1-a meta-analysis of 15 prospective cohort studies. N Engl J Med 1999;340:977-987.
23. Committee on Obstetric Practice. ACOG committee opinion scheduled Cesarean delivery and the prevention of vertical transmission of HIV infection. Number 234, May 2000 (replaces number 219, August 1999). Int J Gynaecol Obstet 2001;73:279-281.
Table 1
CDC Recommendations for sexually transmitted infection (STI) screening in pregnancy
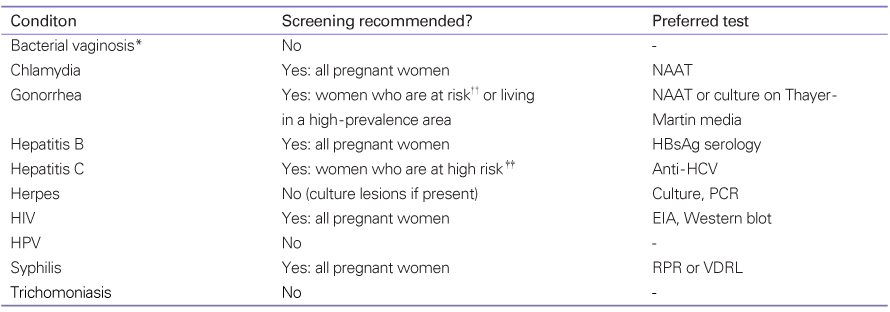
"Yes" indicates screening is recommended at the first prenatal visit, with repeat screening in the third trimester for those at risk.
CDC: Centers for Disease Control and Prevention; NAAT: nucleic acid amplification test; HBsAg: hepatitis B surface antigen; HCV: hepatitis C virus; PCR: polymerase chain reaction; HIV: human immunodeficiency virus; EIA: enzyme immunoassay; HPV: human papillomavirus; RPR: rapid plasma reagin; VDRL: Venereal Disease Research Laboratories.
*Bacterial vaginosis is not an STI, but it is more common in sexually active women.
††Women who have a new or more than one sex partner.
‡‡Women with a history of injection drug use, repeated exposure to blood products, or blood transfusion or organ transplant before 1992.
Table 2
Recommended treatment for pregnant women for syphilis
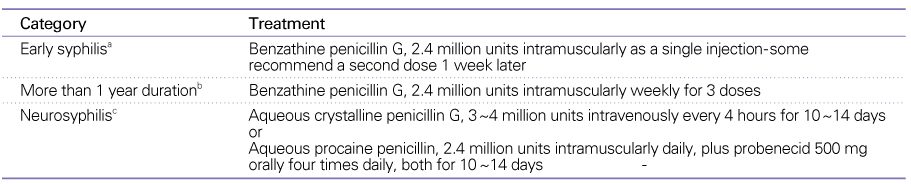
aPrimary, secondary, and latent syphilis of less than 1 year duration.
bLatent syphilis of unknown or more than 1 year duration; tertiary syphilis.
cSome recommend benzathine penicillin, 2.4 million units intramuscularly after completion of the neurosyphilis treatment regimens.
From the Centers for Disease Control and Prevention (5).
Table 3
Pediatric AIDS clinical trials group (PATCG) 076 zidovudine regimen

aAcceptable alternative regimens include 200 mg three times daily or 300 mg twice daily.
bFor elective cesarean delivery, intravenous zidovudine is begun at least 3 hours prior to surgery. For premature rupture of membranes or labor with a planned operative delivery, the loading dose may be given during 30 minutes prior to surgery.
cIntravenous dosage for infants who cannot tolerate oral intake is 1.5 mg/kg intravenously every 6 hours.
From U.S. Public Health Service, 2003. (21)
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,318 View
- 9 Download
-

-
Related articles in
J Korean Med Assoc -
Management of cardiovascular disease in patients with schizophrenia2024 February;67(2)
Hypertension, Proteinuria during Pregnancy1998 April;41(4)
Management of Prostate Disorder in Aging Male1998 September;41(9)
Pharmacologic Management of Rheumatic Diseases2000 April;43(4)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
