





 |
 |
| J Korean Med Assoc > Volume 61(9); 2018 > Article |
Hyun Jung Kim, MD1 , Yeon-Mok Oh, MD2
, Yeon-Mok Oh, MD2
, Yeon-Mok Oh, MD2
Abstract
Chronic obstructive pulmonary disease (COPD) should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease, such as cigarette smoking, biomass exposure, and occupational dust. Spirometry is required to make the diagnosis, and a post-bronchodilator forced expiratory volume in one second/forced vital capacity ratio <0.7 confirms the presence of persistent airflow limitation. The goal of COPD assessment is to determine the severity of the disease, including the severity of airflow limitation, the impact of the disease on the patient's health status, the risk of future events (such as exacerbations, hospital admission, or death), and comorbidities in order to guide therapy. Concomitant chronic diseases occur frequently in COPD patients, including cardiovascular disease, skeletal muscle dysfunction, metabolic syndrome, osteoporosis, depression, anxiety, and lung cancer. These comorbidities should be actively surveilled and treated appropriately when present, as they can independently influence mortality and hospitalization. Above all, further efforts are required to increase the diagnosis rate of COPD in Korea.
References
1. Pauwels RA, Rabe KF. Burden and clinical features of chronic obstructive pulmonary disease (COPD). Lancet 2004;364:613-620.


2. Yoo KH, Kim YS, Sheen SS, Park JH, Hwang YI, Kim SH, Yoon HI, Lim SC, Park JY, Park SJ, Seo KH, Kim KU, Oh YM, Lee NY, Kim JS, Oh KW, Kim YT, Park IW, Lee SD, Kim SK, Kim YK, Han SK. Prevalence of chronic obstructive pulmonary disease in Korea: the fourth Korean National Health and Nutrition Examination Survey, 2008. Respirology 2011;16:659-665.
3. Yoon HK, Park YB, Rhee CK, Lee JH, Oh YM. Committee of the Korean COPD Guideline 2014. Summary of the chronic obstructive pulmonary disease clinical practice guideline revised in 2014 by the Korean Academy of Tuberculosis and Respiratory Disease. Tuberc Respir Dis (Seoul) 2017;80:230-240.


4. Korea Academy of Tuberculosis and Respiratory Diseases. COPD clinical practice guidelines revised in 2018 [Internet] Seoul: Korean Academy of Tuberculosis and Respiratory Disease. 2018;cited 2018 Sep 1. Available from: http://www.lungkorea.org/bbs/?code=guide
5. Woodruff PG, Barr RG, Bleecker E, Christenson SA, Couper D, Curtis JL, Gouskova NA, Hansel NN, Hoffman EA, Kanner RE, Kleerup E, Lazarus SC, Martinez FJ, Paine R 3rd, Rennard S, Tashkin DP, Han MK. SPIROMICS Research Group. Clinical significance of symptoms in smokers with preserved pulmonary function. N Engl J Med 2016;374:1811-1821.
6. Eisner MD, Blanc PD, Yelin EH, Katz PP, Sanchez G, Iribarren C, Omachi TA. Influence of anxiety on health outcomes in COPD. Thorax 2010;65:229-234.
7. Wagner PD. Possible mechanisms underlying the development of cachexia in COPD. Eur Respir J 2008;31:492-501.
8. Schunemann HJ, Dorn J, Grant BJ, Winkelstein W Jr, Trevisan M. Pulmonary function is a long-term predictor of mortality in the general population: 29-year follow-up of the Buffalo Health Study. Chest 2000;118:656-664.
9. Chung KS, Jung JY, Park MS, Kim YS, Kim SK, Chang J, Song JH. Cut-off value of FEV1/FEV6 as a surrogate for FEV1/FVC for detecting airway obstruction in a Korean population. Int J Chron Obstruct Pulmon Dis 2016;11:1957-1963.
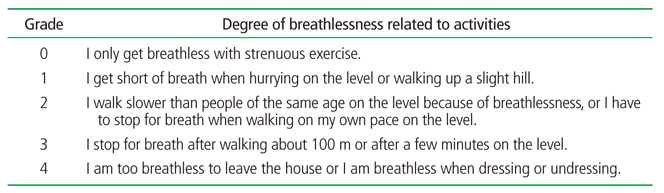
10. Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest 2002;121:1434-1440.
11. Korea Academy of Tuberculosis and Respiratory Diseases. Resource center: mMRC [Internet] Seoul: Korean Academy of Tuberculosis and Respiratory Disease. 2018;cited 2018 Sep 8. Available from: Korean http://www.lungkorea.org/calculator/?code=mmrc
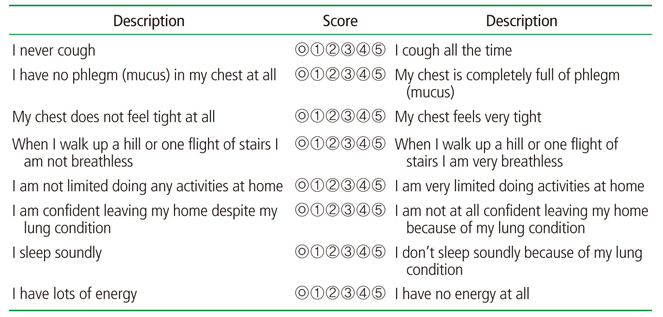
12. Lee S, Lee JS, Song JW, Choi CM, Shim TS, Kim TB, Cho YS, Moon HB, Lee SD, Oh YM. Validation of the Korean version of chronic obstructive pulmonary disease assessment test (CAT) and dyspnea-12 questionnaire. Tuberc Respir Dis 2010;69:171-176.
13. Lee SD, Huang MS, Kang J, Lin CH, Park MJ, Oh YM, Kwon N, Jones PW, Sajkov D. Investigators of the Predictive Ability of CAT in Acute Exacerbations of COPD (PACE) Study. The COPD assessment test (CAT) assists prediction of COPD exacerbations in high-risk patients. Respir Med 2014;108:600-608.
14. Korea Academy of Tuberculosis and Respiratory Diseases. Resource center: CAT [Internet] Seoul: Korean Academy of Tuberculosis and Respiratory Disease. 2018;cited 2018 Sep 8. Available from: http://www.lungkorea.org/calculator/?code=cat
15. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation: the St. George's respiratory questionnaire. Am Rev Respir Dis 1992;145:1321-1327.
16. Burge S, Wedzicha JA. COPD exacerbations: definitions and classifications. Eur Respir J Suppl 2003;41:46s-53s.
17. Hurst JR, Vestbo J, Anzueto A, Locantore N, Mullerova H, Tal-Singer R, Miller B, Lomas DA, Agusti A, Macnee W, Calverley P, Rennard S, Wouters EF, Wedzicha JA. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med 2010;363:1128-1138.
18. Kim MH, Lee K, Kim KU, Park HK, Jeon DS, Kim YS, Lee MK, Park SK. Risk factors associated with frequent hospital readmissions for exacerbation of COPD. Tuberc Respir Dis 2010;69:243-249.
19. Joo H, Park J, Lee SD, Oh YM. Comorbidities of chronic obstructive pulmonary disease in Koreans: a population-based study. J Korean Med Sci 2012;27:901-906.
20. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J 2008;32:962-969.
Figure 1
COPD-6. A chronic obstructive pulmonary disease screening device measuring forced expiratory volume in one second and forced expiratory volume in six seconds (courtesy of Vitalograph).

Figure 2
Combined chronic obstructive pulmonary disease assessment (forced expiratory volume in one second [FEV1], symptom, acute exacerbation). Group (Ga): low risk, low symptom. FEV1 ≥60% of predicted value and no or one exacerbation in previous year, modified Medical Research Council (mMRC) 0 to 1 (or COPD Assessment Test [CAT] <10). Group (Na): low risk, high symptom. FEV1 ≥60% of predicted, no acute exacerbation or one in previous year, mMRC ≥2 (or CAT ≥10). Group (Da): high risk. Regardless of mMRC or CAT score, FEV1 <60% of predicted value or two acute exacerbation or one admission history related to acute exacerbation.
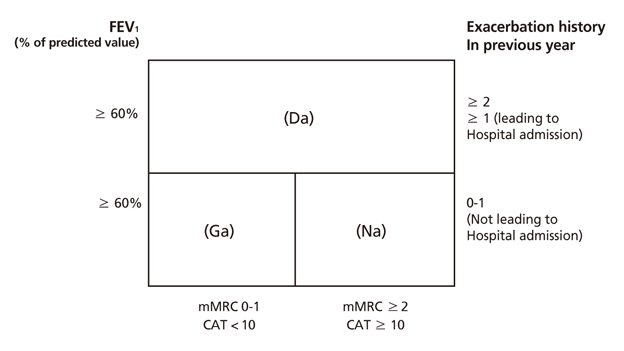
Table 1
Key indicators for considering the diagnosis of COPD

Considering COPD, and perform spirometry, if any of these indicators are present in an individual over age 40. These factors are not diagnostic themselves, but the presence of multiple key indicators increases the probability of the diagnosis of COPD. Spirometry is required to establish the diagnosis of COPD. Reproduced from Korea Academy of Tuberculosis and Respiratory Diseases. COPD clinical practice guidelines revised in 2018 [Internet]. Seoul: Korean Academy of Tuberculosis and Respiratory Disease; 2018, with permission from Korea Academy of Tuberculosis and Respiratory Diseases [4].
COPD, chronic obstructive pulmonary disease.
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Updated view on the treatment of chronic obstructive pulmonary disease in Korea2021 March;64(3)
Anesthetic management of patients with chronic obstructive pulmonary disease2020 September;63(9)
Pharmacotherapy of Chronic Obstructive Pulmonary Diseases1998 April;41(4)
Definition, Epidemiology and Pathogenesis of Chronic Obstructive Pulmonary Disease2006 April;49(4)
Pathophysiology of Chronic Obstructive Pulmonary Disease2006 April;49(4)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
