Ultrasonography of the Acute Abdomen
Article information
J Korean Med Assoc. 2007;50(1):73-79
Publication date (electronic) : 2007 January 31
doi :
https://doi.org/10.5124/jkma.2007.50.1.73
Abstract
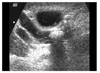
The initial radiologic evaluation of a patient with acute abdominal symptoms begins with plain abdominal radiographs. Plain abdominal radiographs are helpful for the diagnosis of intestinal obstruction and pneumoperitoneum. However, cross-sectional imaging modalities, such as ultrasonography or computed tomography, are necessary for specific diagnosis of acute abdomen. Ultrasonography is a non-invasive and comfortable tool for patients visiting emergency room. This article describes the ultrasonographic findings of most common diseases presenting with acute abdominal symptoms.
Keywords: Abdomen, US; Abdomen, Acute conditions; Ultrasound(US)
References
1. Davies AH, Mastorakou I, Cobb R, Rogers C, Lindsell D, Mortensen NJM. Ultrasonography in the acute abdomen. Br J Surg 1991. 781178–1180.
2. Laing FC. Ultrasonography of the acute abedomen. Radiol Clin North Am 1992. 30389–404.
3. Heller MB, Verdile VP. Ultrasonography in emergency medicine. Emerg Med Clin North Am 1992. 1027–46.
4. Hudson PA, Promes SB. Abdominal ultrasonography. Emerg Med Clin North Am 1997. 15825–848.
5. Cosgrove D, Meire H, Dewbury K. Abdominal and general ultrasound 1994. 1st edth ed. Churchill Livingstone;
6. Lim JH, Kim PN, et al. Abdominal Radiology 2005. 1st edth ed. Seoul: Korean Society of Abdominal Radiology;
7. O'Malley M, Wilson SR. US of gastrointestinal tract abnormalities with CT correlation. Radiographics 2003. 2359–72.
8. Vijayaraghavan SB. High-resolution sonographic spectrum of diverticulosis, diverticulitis, and their complications. J Ultrasound Med 2006. 2575–85.
9. Baker JA, Mandavia D, Swadron SP. Diagnosis of diverticulitis by bedside ultrasound in the emergency department. J Emerg Med 2006. 30327–329.
10. Singh AK, Gervais DA, Hahn P, Sagar P, Mueller PR, Novelline RA. Acute epiploic appendatitis and its mimics. Radiographics 2005. 251521–1534.
11. Hollerweger A, Macheiner P, Rettenbacher T, Gritzmann N. Primary epiploic appendagitis: sonographic findings with CT correlation. Journal Clinical Ultrasound 2002. 30481–495.
12. Buljevac M, Busic Z, Cabrijan Z. Sonographic diagnosis of gallstone ileus. J Ultrasound Med 2004. 231395–1398.
13. Lassandro F, Gagliardi N, Scuderi M, Pinto A, Gatta G, Mazzeo R. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol 2004. 5023–29.
14. Zubaidi A, Al-Saif F, Silverman R. Adult intussusception: A retrospective review. Dis Colon Rectum 2006. 491–6.
15. Mateen MA, Saleem S, Rao PC, Gangadhar V, Reddy DN. Transient small bowel intussusception: ultrasound findings and clinical significance. Abdom Imaging 2006. 301–7.
Article information Continued
Copyright © 2007 Korean Medical Association