





 |
 |
| J Korean Med Assoc > Volume 48(9); 2005 > Article |
Abstract
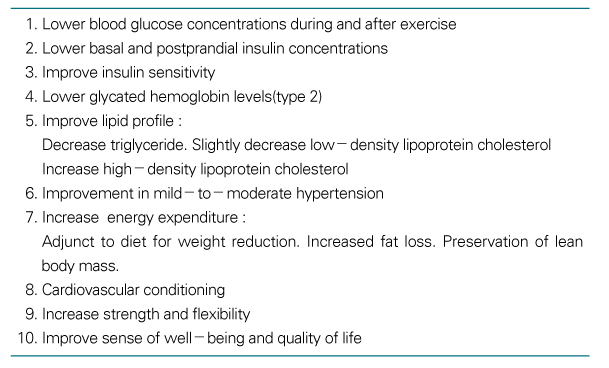
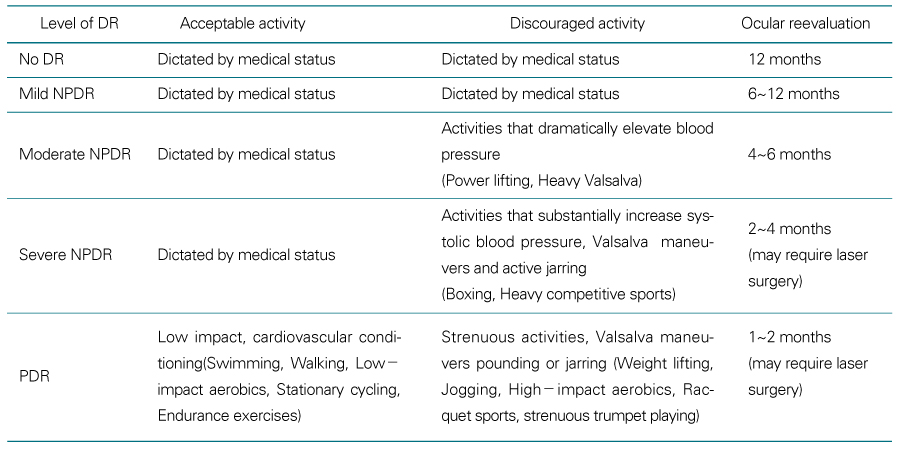
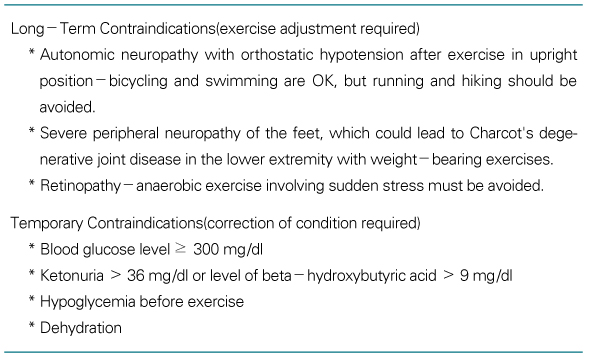
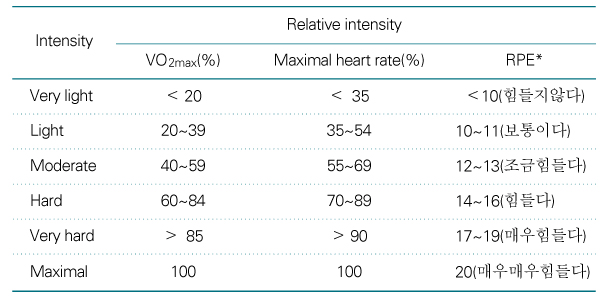
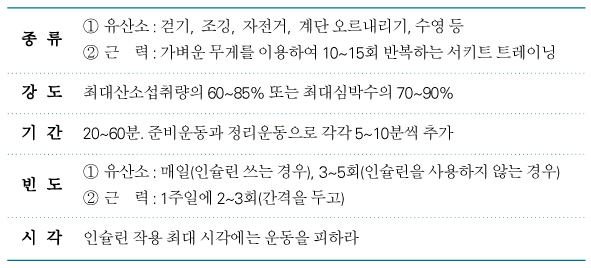
Exercise and diet control are essential for the management of diabetes mellitus. Beneficial effects of exercise have been established. Exercises improve the control of glucose level, decrease cardiac risk factors and prevent type 2 diabetes mellitus. Exercise can cause hypoglycemia or hyperglycemia, cardiac attack, dehydration, foot problems and aggravation of diabetic complications. Pre-exercise medical evaluation is needed to prevent the unwanted effect of exercise. Diabetic patients who have ketonuria and high blood glucose level(more than 250mg/dL) should postpone exercise until the problems are solved. Diabetic patients should enjoy their activities and do warming up and cool down exercise. Vigorous aerobic exercise, 60~85% of maximal oxygen uptake, 20~60 minutes at a time, 3~5 times a week is recommended. Moderate aerobic exercise, 40~60% of maximal oxygen uptake, more than 30 minutes at a time, over 5 times a week is also recommended instead. Muscle strengthening exercises, 2~3 times a week should be added. To prevent hypoglycemia during exercise, the dose of insulin should be reduced. If the patient suffer from hypoglycemic symptom, he or she should take glucose immediately. Therefore diabetic patients should carry some simple carbohydrates. To prevent dehydration during exercise, proper hydration and clothes must be prepared. Wearing well fitting shoes, frequent check up for any wounds on foot are needed to prevent diabetic foot complications. Diabetic patients have the rights to have good quality of life. Regular proper exercise could improve their quality of life.
References
1. Fahey PJ, Stallkamp ET, Kwatra S. The athlete with type I Diabetes: managing insulin, diet and exercise. American Family Physician 1996;53:1611-1617.
2. Boule NG, Haddad E, Kenny GP, Wells GA, Siga RJ. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials. JAMA 2001;286:1218-1227.
3. Eriksson J, Taimela S, Esiksson K. Resistance training in the treatment of non-insulin-dependent diabetes mellitus. Int J Sports Med 1997;18:242-246.
4. Ivy JL. Role of exercise training in the prevention and treatment of insulin resistance and non-insulin-dependent diabetes mellitus. Sports Med 1997;24:321-336.
5. Signal RJ, Wasserman DH, Kenny GP, Castaneda-Sceppa C. Physical activity/exercise and type 2 diabetes. Diabetic care 2004;27:2518-2539.
6. Lebovitz HE. Therapy for Diabetes Mellitus and related Disorders 1994;2nd ed. Alexandria: American Diabetes Association, Inc.. 107-115. ed Exercise.
7. Pan XR, Li GW, Wang JX, Uang WY, An ZX, Howard BV, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance: the Da Qing IGT and Diabetes Study. Diabetes Care 1997;20:537-544.
8. Lindstrom J, Louheranta A, Mannein M, Rastas M, Salminen V, Tuomilehto J, et al. The Finnish Diabetes Prevention Study( DPS) : lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care 2003;26:3230-3236.
9. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Eng J Med 2002;346:393-403.
10. Diabetes Prevention Program Research Group. The Diabetes Prevention Program(DPP): description of lifestyle intervention. Diabetes Care 2002;25:2165-2171.
11. Eriksson KF, Lindgarde F. No excess 12-year mortality in men with impaired glucose tolerance who participated in the Malmo Prevention trial with diet and exercise. Diabetologia 1998;41:1010-1016.
12. Sato Y, Iguchi A, Sakamoto N. Biochemical determination of training effects using insulin clamp technique. Horm Metb Res 1984;16:483-486.
13. American diabetes association. International Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183-1197.
14. Albright AL. In: Wikgren S, editor. Diabetes. ACSM's Exercise Management for Persons with Chronic Diseases and Disabilities 1997;Champaign: Human Kinetics. 94-100.
15. In: McArdle WD, Katch FI, et al, editor. Exercise physiology 1996;4th ed. Baltimore: Williams & Wilkins. 372-377.
16. Diabetes medical guidelines task force. AACE diabetes guidelines. Endocr Pract 2002;8:Suppl 1. 41-73.
17. Devlin JT, Ruderman N. Diabetes and exercise: the risk-benefit profile. The Health Professional's Guide to Diabetes and Exercise 1995;Alexandria: American Diabetes Association. 3-4.
18. American diabetes association. Physical activity/exercise and diabetes mellitus. Diabetic care 2003;26:Suppl. S73-S77.
19. Campaign BN. Exercise and diabetes mellitus. ACSM's guidelines for exercise testing and prescription 2000;6th ed. Philadelphia: Lippincott Williams & Wilkins. 277-284.
- TOOLS
-
- Share :
-





-
METRICS

-
- 1 Crossref
- Scopus
- 1,166 View
- 9 Download
-

-
Related articles in
J Korean Med Assoc -
Exercise therapy for diabetes mellitus2023 July;66(7)
Diagnosis and management of gestational diabetes mellitus2023 July;66(7)
Pharmacotherapy for patients with diabetes mellitus2020 December;63(12)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
