






 |
 |
| J Korean Med Assoc > Volume 47(11); 2004 > Article |
Abstract
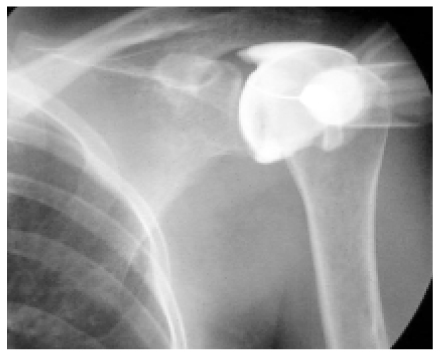
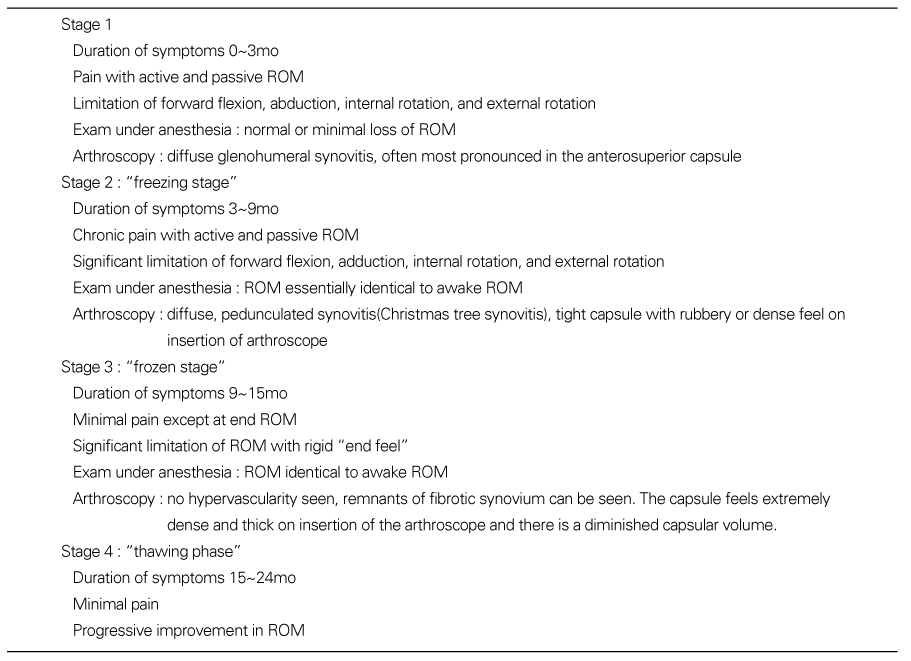
Adhesive capsulitis was described initially as periarthritis, and then frozen shoulder. Adhesive capsulitis of the shoulder is an insidious, painful condition that results in a gradual restriction of movements. Adhesive capsulitis can be classified into primary or secondary. Primary adhesive capsulitis is an insidious condition, whereas secondary adhesive capsulitis is associated with a known pathology. The pathogenesis remains unclear. Gross pathological changes include thickening and constriction of the capsule, especially anterioinferiorly with a very little amount of synovial fluid in the joint space. Many patients continue to have a significant long-term restriction in their range of motion, although few are functionally restricted. Classically adhesive capsulitis is divided into three phases : the painful phase, the stiff phase, and the resolution phase. The diagnosis of adhesive capsulitis is based on a thorough history taking and physical examination. Radiographs of the shoulder are usually negative. An arthrogram may show a decrease in the intraarticular volume and an absence of the axillary recess. The final confirmation of the diagnosis is made by an experience of relief of pain following an intra-articular anesthetic. Prevention is the ideal treatment. The goals of treatment are to relieve pain, to restore motion, and to restore function. Treatment modalities include anti-inflammatory medications, physical therapy including therapeutic exercise, corticosteroid injection, suprascapular nerve block, capsular distension, manipulation under anesthesia, and arthroscopic capsular release. It is necessary to refine the selection of treatment for individual patients according to the phase of the disease.
References
1. Neviaser JS. Adhesive capsulitis of the shoulder: a study of the pathologic findings in periarthritis of the shoulder. J Bone Joint Surg 1945;27:211-222.
2. Lundberg BJ. The frozen shoulder: clinical and radiographical observations:the effect of manipulation under general anesthesia: structure and glycosaminoglycan content of the joint capsule. Acta Orthop Scand 1969;119:1-59.
3. McLaughlin HL. On the "frozen" shoulder. Bull Hosp Joint Dis 1951;12:383-393.
4. Rodeo SA, Hannafin JA, Tom J, Warren RF, Wickiewicz TC. Immunolocalization of cytokines and their receptor in adhesive capsulitis of the shoulder. J Orthop Res 1997;15:427-436.
5. Binder AI, Bulgen DY, Hazelman BL, Robers S. Frozen shoulder: a long-term prospective study. Ann Rheum Dis 1984;43:361-364.
6. Neviaser RJ, Neviaser TJ. Arthroscopy of the shoulder. Orthop Clin North Am 1987;18:369-370.
7. Hannafin JA, Chiaia TA. Adhesive capsulitis:a treatment approach. Clin Orthop 2000;372:95-109.
8. Reeves B. The natural history of the frozen shoulder syndrome. Scand J Rheumatol 1975;4:193-196.
10. Ryu KN, Lee SW, Rhee YG, Lim JH. Adhesive capsulitis of the shoulder joint: usefulness of dynamic sonography. J Ultrasound Med 1993;12:445-449.
11. Binder AI, Bugen DY, Hazleman BL, Tudor J. Frozen shoulder: an arthographic and radionuclear scan assessment. Ann Rheum Dis 1984;43:365-369.
12. Neviaser TJ. Adhesive capsulitis. Orthop Clin North Am 1987;18:439-443.
13. Hollingworth GR, Ellis R, Haggersley TS. Comparison of injection techniques for frozen shoulder pain:results of a double-blind, randomized study. BMJ 1983;287:1339-1341.
14. Dacre JE, Beeney N, Scott DC. Injections and physiotherapy for the painful stiff shoulder. Ann Rheum Dis 1989;48:322-325.
15. Rizk TE, Christopher RP, Pinals RS. Treatment of adhesive capsulitis(frozen shoulder): a new approach to its management. Arch Phys Med Rehabil 1983;64:29-33.
16. Vad VB, Sakalkale D, Warren RF. The role of capsular distension in adhesive capsulitis. Arch Phys Med Rehabil 2003;84:1290-1292.
17. Rizk TE, Gavant ML, Pinals RS. Treatment of adhesive capsulitis(frozen shoulder) with arthrographic capsular distension and rupture. Arch Phys Med Rehabil 1994;75:803-807.
18. Gam AN, Schydlowsky P, Rossel I, Remvig L, Jensen EM. Treatment of "frozen shoulder" with distension and glucocorticoid compared with glucocorticoid alone. Scand J Rheumatol 1998;27:425-430.
20. Fareed DO, Gallivan WR Jr. Office management of frozen shoulder syndrome: Treatment with hydraulic distension under local anesthesia. Clin Orthop 1989;242:177-183.
22. Karatas GK, Meray J. Suprascapular nerve block for pain relief in adhesive capsulitis:comparison of 2 different techniques. Arch Phys Med Rehabil 2002;83:593-597.
23. Warner JP. Frozen shoulder: diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140.
24. Janda DH, Hawkins RJ. Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus:a clinical note. J shoulder Elbow Surg 1993;2:36-38.
25. Kivimaki J, Pohjolainen T. Manipulation under anesthesia for frozen shoulder with and without steroid injection. Arch Phys Med Rehabil 2001;82:1188-1190.
26. Warner JP, Allen A, Marks PH, Wong P. Arthroscopic release for chronic, refractory adhesive capsulitis of the shoulder. J Bone Joint Surg Am 1996;78:1808-1816.
- TOOLS
-
- Share :
-





-
METRICS

-
- 5 Crossref
- Scopus
- 1,167 View
- 50 Download
-

-
Related articles in
J Korean Med Assoc -
Diagnosis and treatment of adult spinal deformity2023 August;66(8)
Diagnosis and treatment of trigeminal neuralgia2023 January;66(1)
Diagnosis and Medical Treatment of Seronegative Spondyloarthropathy1997 January;40(1)
Diagnosis and Treatment of Chronic Congestive Heart Failure1997 November;40(11)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
