





 |
 |
| J Korean Med Assoc > Volume 47(3); 2004 > Article |
Abstract
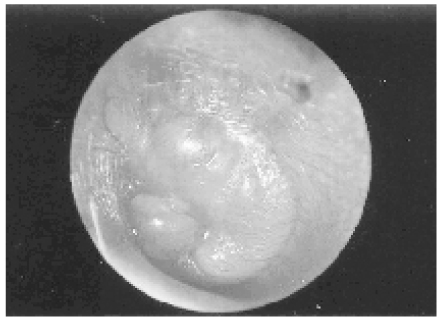
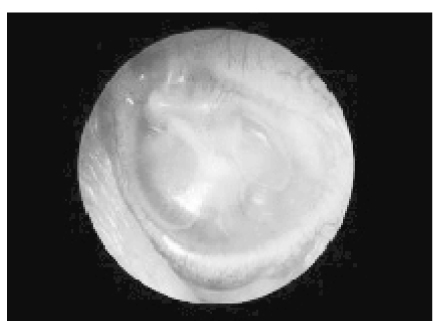
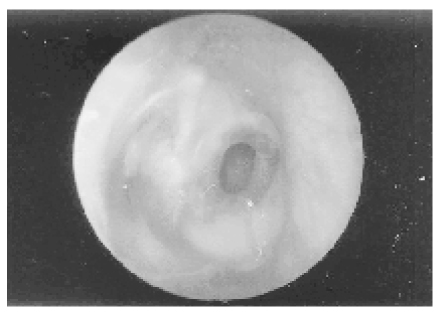
Otitis media is one of the most common diseases during childhood with a peak incidence and prevalence from 6 to 20 months of age. It is the most frequent disease managed with antibiotics in children. The infection typically develops as a result of bacterial contamination through the Eustachian tube in the presence of preexisting inflammation in the middle ear. The optimal method of management remains open to question and is the subject of continuing controversy. Over-diagnosis of the disease and unnecessary prescription of antibiotics for this condition have contributed to the spread of antimicrobial resistance. Thus, the differential diagnosis between acute otitis media and otitis media with effusion is important to determine the management strategy ; whether to use antibiotics and which antibiotics to use when necessary. Otitis media may be accompanied by a variable degree of conductive hearing loss. Both infectious and noninfectious complications of otitis media may result in significant morbidity and complications, including acute and chronic mastoiditis, petrositis, and intracranial infection.
References
1. Rutka J, Lekagul S. No therapy:use, abuse, efficacy, and morbidity-the European versus the Third-World experience. J Otolaryngol 1998;27:Suppl 2. 43-48.
2. Gates GA. In: Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Richardson MA, Scculler DE, editor. Acute otitis media and otitis media with effusion. Otolaryngology Head & Neck Surgery 1998;3rd ed. Mosby Co. 461-477.
3. Rosenfeld RM. An evidence-based approach to treating otitis media. Pediatr Clin North Am 1996;43:1165-1181.
4. Little P, Gould C, Williamson I, Moore M, Warner G, Dunleavey J. Pragmatic randomised controlled trial of two prescribing strategies for childhood acute otitis media. BMJ 2001;322:336-342.
5. Froom J, Culpepper L, Jacobs M, DeMelker RA, Green LA, Heeren T, et al. Antimicrobials for acute otitis media:A review from the International Primary Care Network. BMJ 1997;315:98-102.
6. Dowell SF, Butler JC, Giebink GS, Jacobs MR, Jernigan D, Schwartz B, et al. Acute otitis media:management and surveillance in an era of pneumococcal resistnace-a report from the Drug-resistant Streptococcus pneumoniae Therapeutic Working Group. Pediatr Infect Dis J 1999;18:1-9.
7. Bitnun A, Allen UD. Medical therapy of otitis media: use, abuse, efficacy, and morbidity. J Otolaryngol 1998;27:Suppl 2. 26-36.
8. Williams RL, Chalmers TC, Stange KC, Chalmers FT, Bowlin SJ. Use of antibiotics in preventing recurrent otitis media and in treating otitis media with effusion:a meta-analytic attempt to resolve the brouhaha. JAMA 1993;270:1344-1351.
9. Alho OP, Läärä E, Oja H. What is the natural history of recurrent acute otitis media in infancy? J Fam Pract 1996;43:258-264.
10. Rosenfeld RM, Vertrees JE, Carr J, Cipolle RJ, Uden DL, Canafax DM, et al. Clinical efficacy of antimicrobial drugs for acute otitis media:meta-analysis of 5400 children from thirty-three randomized trials. J Pediatr 1994;124:355-367.
11. Schwartz RH, Rosenberg WJ, Schwartz DM. Office myringotomy for acute otitis media:its value in preventing middle ear effusion. Laryngoscope 1981;91:616-619.
12. American Academy of Pediatrics The Otitis Media Guideline Panel. Managing otitis media with effusion in young children. Pediatrics 1994;94(5):766-773.
Table 1

* For children who are allergic to penicillin, preferred alternatives include cefuroxime axetil or another second-generation cephalosporin(other than cefaclor, which may cause a serum sickness like reaction), azithromycin, or ceftriaxone(50mg/kg once)
† The delayed antibiotic prescribing strategy is as follows : initiate treatment with full-dose acetaminophen ; provide a prescription for amoxicillin to be used only if otalgia or fever persist or if there is no clinical improvement after 48 to 72 hours ; advise the patient's parent that antibiotics do not work very well against otitis and have virtually no effect during the first 24 hours ; explain the disadvantages of antibiotics to patient's parents-they may have side effects(e.g., diarrhea and rash) ; and select for resistant bacteria
Table from Hendley JO. Otitis media. N Engl J Med 2002 ; 347(15) : 1169 - 74
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,171 View
- 4 Download
-

-
Related articles in
J Korean Med Assoc -
Diagnosis and treatment of dyslipidemia in children and adolescents2024 May;67(5)
Management of cardiovascular disease in patients with schizophrenia2024 February;67(2)
Management of post-cardiac arrest syndrome2023 September;66(9)
Management of patients with neuropathic pain2022 August;65(8)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
