서론
위암은 전 세계적으로 5번째로 흔한 종양이며, 3번째의 암사망 원인으로 매년 951,000명의 환자가 발생하고, 723,000명이 위암으로 사망한다[1]. 국내에서는 1년에 약 32,000명의 새로운 환자가 발생하여 2번째로 흔한 종양이며, 폐암 및 간암에 이어 3번째의 암사망 원인이다[2]. 서양에서 위암은 진단 당시 진행된 병기가 많아 예후가 불량하여 5년 생존율이 20-30% 내외에 불과하다[3,4]. 이에 비하여 우리나라나 일본에서는 국가 조기검진의 시행으로 조기 위암의 발견이 많아지면서 5년 생존율이 향상되어 60-70%에 이르고 있다[2,3].
전이성 위암 또는 수술 후 재발한 위암 환자에서는 항암화학요법이 주된 치료가 된다. 지난 30여 년간 전이성 위암에 대한 항암화학요법은 상당히 발전되어 과거에 비해 생존기간이 뚜렷하게 개선되었지만 아직도 전이성 위암 환자의 전체생존기간은 12개월을 약간 넘는 수준에 불과한 실정이다[5]. 최근 trastuzumab 및 ramucirumab 등 표적치료제가 위암 치료에 도입이 되면서 위암 환자의 생존기간이 연장되고 있으며 새로운 표적치료제를 이용한 임상연구가 매우 활발히 진행되고 있다. 본 종설에서는 전이성 위암에서의 항암요법의 현황에 대해 살펴보고 앞으로의 발전 전망을 논하고자 한다.
1차 항암요법
1. 세포독성항암제
전이성 위암에서 치료의 근간은 항암화학요법이다. 항암화학요법이 전이성 위암 환자의 생명을 연장하고 삶의 질을 향상시키는지에 대해서는 더 이상의 이론은 없는 상태이다 (hazard ratio [HR], 0.39; 95% confidence interval [CI], 0.28 to 0.52) [4].
전이성 위암 환자에서는 fluoropyrimidine계 항암제 (5-fluorouracil [5-FU], capecitabine, TS-1), anthracycline계(epirubicin, doxorubicin), platinum계(cisplatin, oxaliplatin), taxane계(docetaxel, paclitaxel) 및 topoisomerase I 억제제(irinotecan) 등이 널리 사용되고 있다. 이들 약제들을 병용하여 치료하는 복합치료와 단독치료를 비교한 메타분석에서는 단독치료에 비해 복합치료군에서 향상된 종양반응률(35% vs. 18%) 및 유의한 생존 기간의 연장(HR, 0.83; 95% CI, 0.74 to 0.93)을 보여주어 환자의 전신상태가 괜찮다면 우선적으로 복합 항암화학요법을 고려해야 한다[6].
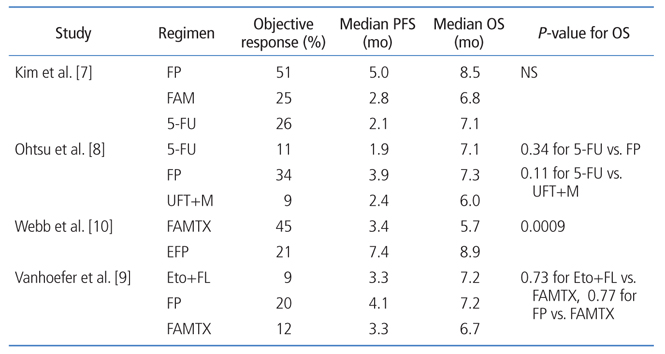
우리나라에서는 일찍이 Kim 등[7]이 5-FU와 cisplatin 복합요법(5-fluorouracil+cisplatin [FP]요법)을 5-FU 단독과 5-FU, doxorubicin, mitomycin-C 등과 비교하여 종양반응률이나, 무진행생존기간(progression-free survival, PFS)이 우월함을 보고하였다. 이 연구에서 환자들의 전체생존기간이 통계적으로 유의한 만큼 연장되지는 않았지만, FP요법은 우리나라를 비롯한 여러 나라에서 가장 널리 사용되는 치료의 하나가 되었다. 1990년대에 다른 나라에서 시행된 3상 임상시험은 Table 1과 같으며, 거의 유사한 결과를 보여주었다[7,8,9,10].
2000년대 들어서면서 5-FU의 새로운 경구용 약제(capecitabine 및 TS-1), oxaliplatin, taxane계 항암제 그리고 irinotecan 등이 위암의 치료에 시험되었다. Table 2에 보는 것처럼 capecitabine 또는 TS-1은 5-FU와 비슷한 효과를 보여주었으며, oxaliplatin도 cisplatin과 동등한 결과를 나타내었다[11,12,13,14,15]. Capecitabine 및 TS-1은 경구로 편리하게 투여할 수 있으며, oxaliplatin은 신기능 보전을 위한 별도의 보조치료가 필요 없다는 점에서 환자에게 투여의 편익을 제공할 수 있다.
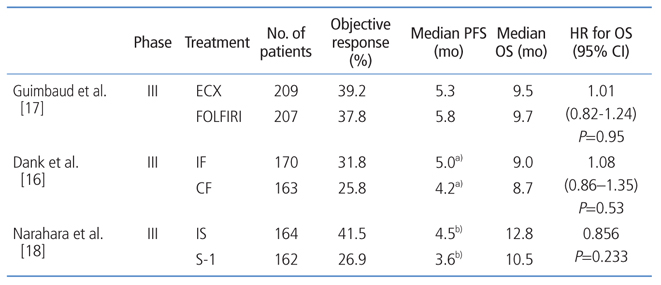
한편, 5-FU/leucovorin/irinotecan 또는 TS-1/irinotecan 등 cisplatin을 포함하지 않은 요법도 시도되었는데, Table 3에서 나타난 바와 같이 cisplatin 포함 복합 항암화학요법과 비슷한 임상적 효과를 보여주었다[16,17,18]. 전이성 위암 환자의 생존기간을 더 연장시키기 위하여 5-FU/platinum에 docetaxel을 추가한 docetaxel/5-FU/cisplatin 요법이 시행되었는데 비록 전체생존기간은 향상시켰지만(9.2개월 vs. 8.6개월; HR, 1.29; 95% CI, 1.0 to 1.6; P=0.02), grade III/IV의 과립구감소증과 발열 또는 설사가 각각 약 30%의 환자에서 관찰되어, 이 연구에서 사용된 용량으로는 별로 사용되고 않고 있다[19]. 유럽에서는 epirubicin을 추가한 epirubicin/cisplatin/5-FU 요법이 널리 사용되어 왔으나, 최근 연구에서 epirubicin/cisplatin/cape-citabine요법이 5-FU/leucovorin/irinotecan 요법에 비해 효과는 비슷하지만, 부작용이 더 많은 것으로 나타났다[17]. 따라서 3제요법은 과도한 독성 등을 고려할 때 2제요법보다 더 낫다고 할 수 없으며 임상 현장에서의 적용에는 신중을 기해야 할 것이다.
2. 표적치료제: HER2 targeted agents
HER2는 human epidermal growth factor receptor (HER family)의 한 종류로 세포막 관통 단백질이며, HER2의 과발현 또는 유전자 증폭은 비정상적인 세포 내 신호전달을 초래하여 세포 증식 및 생존에 관여하는 것으로 알려져 있고, 위암에서의 HER2 과발현 빈도는 연구자마다 차이는 있지만 10% 전후로 보고되고 있다[20,21]. HER2 양성은 면역조직 화학염색에서 강양성(3+) 이거나 또는 중등도 양성(2+)이면서 fluorescence in situ hybridization 양성으로 정의한다. 이러한 HER2를 표적으로 하는 약제에는 HER2 수용체를 차단하는 단클론항체인 trastuzumab, pertuzumab 등이 있고, 저분자물질로 tyrosine kinase 억제제인 lapatinib이 있다.
ToGA 연구에서는 HER2 양성 진행성 위암 환자 594명을 대상으로 항암화학요법(5-FU/cisplatin 또는 capecitabine/cisplatin)군과 항암화학요법에 trastuzumab을 병용한 군을 비교하였는데 trastuzumab 병용군에서 생존기간의 연장(13.8개월 vs. 11.1개월, P=0.0046)은 물론, 반응률 개선과 PFS의 연장을 보여주었다[22]. 이러한 차이는 면역조직화학염색에서 강양성(3+)을 보이거나 또는 중등도 양성 (2+)이면서 fluorescence in situ hybridization 양성인 환자에서 더 뚜렷한 차이를 보여 주었다(16.0개월 vs. 11.8개월, P=0.036). ToGA 연구 결과를 바탕으로 HER2 양성 위암에서 1차 치료로 trastuzumab 병합 항암화학요법이 표준치료가 되었다.
HER2 및 epidermal growth factor receptor (EGFR)의 tyrosine kinase 억제제인 lapatinib은 HER2 양성 위암세포주에서 trastuzumab보다 우월한 항암효과를 보여주었기에 lapatinib도 HER2 양성 전이성 위암에서 시험되었다[23]. LOGiC 연구는 1차 치료로서 HER2 양성 위암환자를 대상으로 XELOX 항암제군과 항암제와 lapatinib 병용군을 비교하였는데 생존기간에서 양 치료군 간에 유의한 차이는 관찰되지 않았다(10.5개월 vs. 12.2개월, P=0.35) [24]. TyTAN 연구에서는 2차 치료로서 HER2 양성 위암환자를 paclitaxel군과 paclitaxel과 lapatinib 병용군으로 나누어 비교분석하였는데 lapatinib 병용군에서 유의한 생존기간의 연장은 보여주지 못하였다(8.9개월 vs. 11.0개월, P=0.1044).
3. 기타 표적치료제
Vascular epidermal growth factor (VEGF) 및 VEGF receptor (VEGFR)는 혈관신생에 관여하는 인자로 위암발생에 중요한 인자 중 하나로 알려져 있다. Bevacizumab은 VEGF-A에 대한 인간 단클론 항체로 AVAGAST 연구는 1차 항암요법으로 fluoropyrimidine/cisplatin 화학요법과 화학요법에 bevacizumab을 병용한 요법을 비교한 제3상 연구이다[25]. 이 연구에서 bevacizumab 과의 병용요법은 PFS는 연장시켰으나 연구의 1차 목표였던 전체 생존기간은 연장시키지 못하였다(12.1개월 vs. 10.1개월, P=0.1002).
2차 항암요법
전이성 위암에서 1차 항암화학요법이 생존기간을 연장시키나, 아직까지 1차 항암화학요법의 종양반응률은
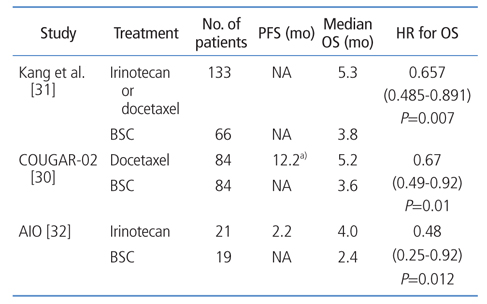
35-50%, PFS는 4-6개월에 불과하다[6,11,12,13,14,15]. 따라서 1차 항암화학요법에 불응하거나 실패한 경우 2차 항암화학요법을 고려할 수 있으며, 최근 2차 항암요법에 대한 몇몇 제3상 연구결과들이 발표되었다(Table 4) [30,31,32]. 국내에서는 irinotecan 또는 docetaxel과 최선의 지지요법을 비교한 3상 연구가 있으며, COUGAR-02는 docetaxel을 그리고 AIO 연구는 irinotecan을 최선의 지지요법과 비교한 3상 연구이다. 상기 3개의 연구 모두에서 2차 항암화학요법은 최선의 지지요법에 비하여 의미 있는 생존기간의 연장을 보여주었으며, 메타분석에서도 2차 항암화학요법을 시행하는 경우 통계적으로 유의한 사망위험도의 감소가 관찰되었다(HR, 0.64; 95% CI, 0.52 to 0.79; P<0.0001) [33]. 따라서 1차 치료에 불응하거나 실패한 전이성 위암에서 2차 항암화학요법은 환자의 전신상태를 고려하여 표준치료로써 시행된다. 그러나 2차 항암화학요법으로 어떤 약제가 더 우월한지에 대해서는 아직까지 명확한 결론이 나지 않은 상태이며, 환자의 전신상태, 이전 치료력 등을 종합적으로 고려하여 2차 항암화학요법 약제를 선택하는 것이 필요하다.
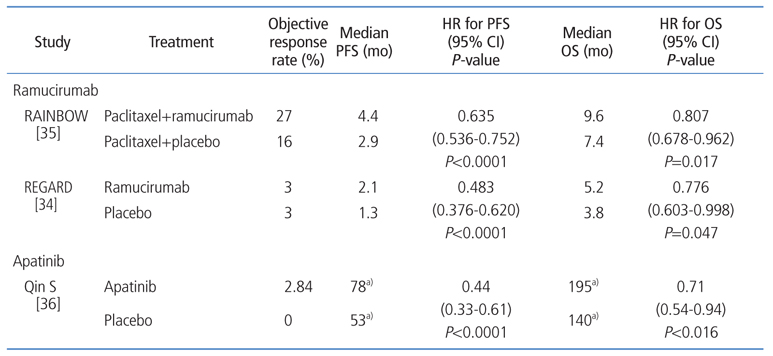
Ramucirumab은 VEGFR-2에 결합하는 인간 IgG1 단클론 항체로 수용체 매개 신호전달체계를 억제하는 것으로 알려져 있으며, 1차 치료에 실패한 전이성 위암 환자를 대상으로 ramucirumab을 이용한 2개의 임상연구 결과가 최근 발표되었다[34,35]. REGARD 연구는 이전에 platinum- 또는 fluoropyrimidine-포함 항암화학요법에 실패한 전이성 위암 환자를 대상으로 시행되었으며, ramucirumab은 위약에 비하여 의미 있는 생존기간의 연장을 보여주었다(Table 5) [34,35,36]. 다른 부작용은 양 치료군 간에 차이는 없었으나 고혈압은 ramucirumab 투여군에서 더 흔하게 관찰되었다. Ramucirumab은 1차 항암화학요법 실패 후 2차 단계에서 사용하여 생존기간을 연장시킨 첫 번째 표적치료제로 그 의의가 있다. RAINBOW 연구는 1차 항암화학요법이 실패한 전이성 위암환자를 대상으로 paclitaxel과 ramucirumab의 병합요법을 paclitaxel 단독과 비교한 제3상 연구이며, 이 연구에서 ramucirumab 병합군은 위약군에 비해 의미 있는 생존기간의 연장이 관찰되었다(Table 5) [34,35,36]. 위의 두 가지 연구에서 ramucirumab은 단독요법 또는 paclitaxel과의 병합치료로 효과가 있음이 밝혀졌으며, 향후 임상 현장에 도입되어 사용될 것으로 기대된다. Apatinib은 저분자 tyrosine kinase 억제제로 VEGFR-2를 표적으로 하며, 이전에 2차 이상의 항암화학요법을 시행받았던 환자를 대상으로 apatinib 단독과 위약을 비교한 제 3상 연구에서 apatinib은 위약에 비하여 의미 있는 생존기간의 연장을 보여주었다[36].
결론
전이성 위암에서 1차 항암화학요법은 생존기간을 연장시키고 삶의 질을 향상시키므로 환자의 전신상태가 양호하다면 표준요법으로 시행되어야 하며, 국내에서는 fluoropyrimidine과 platinum의 병합요법이 가장 흔하게 사용된다. 또한 1차 치료에 실패한 위암 환자에서 2차 항암화학요법은 표준치료이며, 환자의 전신상태에 따라 그 시행을 적극적으로 고려해야 한다. HER2 양성 위암에서 trastuzumab 포함 복합 항암화학요법을 시행해야 하며, 진행성 위암으로 진단 시 먼저 HER2 과발현 여부를 확인하는 것이 매우 중요하다. 최근 혈관신생성장인자와 관련된 ramucirumab의 항암효과에 대한 임상결과가 보고되었으며, 조만간 임상현장에 적용 가능할 것으로 기대가 되고 있다. 현재 진행성 위암 환자를 대상으로 C-MET, PI3K, FGFR 및 immune checkpoint 등과 연관된 여러 새로운 표적치료제에 대한 임상연구가 활발히 진행되고 있으므로 이들 연구결과가 임상 현장에 적용될 경우 향후 환자들의 생존과 삶의 질을 향상시키며, 더 나아가 환자 개개인의 분자적, 유전적 특성에 맞는 치료를 할 수 있을 것으로 전망된다.
Peer Reviewers' Commentary
본 논문은 수술 불가능한 위암의 표준 치료과 현재 진행되고 있는 중요한 임상 연구들의 결과를 다룸으로써 위암 치료의 나아갈 방향을 제시하였고, 유전적 특성에 맞는 맞춤의료의 방향을 요약하였다. 과거에 암으로 진단되면 생존기간이 얼마 되지 않은 것으로 생각되었지만, 최근 새로운 항암제들이 많이 개발되면서 생존기간이 늘어나게 되었고, 암은 당뇨병, 고혈압 등과 마찬가지로 조절하면서 치료하는 만성병 개념으로 되어가고 있다. 논문의 내용은 위암 수술 후 보조요법, 전이성/재발성 위암의 1차 및 2차 치료로 나누어서 근거논문을 중심으로 기술하고 있다. 그리고 최신 치료제인 표적치료제를 소개하고 있어서 위암 치료의 최신 동향을 파악할 수 있는 내용이라고 할 수 있다. 항암치료는 일반적으로 전문 분야로 생각되어 접근하기 어려운 면이 있지만 본 논문을 통하여 일반의사도 쉽게 위암치료의 경향을 알 수 있으리라고 생각된다.
[정리: 편집위원회]