한국의 에딘버러우울척도 활용 현황
Edinburgh Postnatal Depression Scale used in South Korea
Article information

Trans Abstract
Background
The Edinburgh Postnatal Depression Scale (EPDS), a validated screening tool for prenatal and postnatal depression, was included as a reimbursable item by the National Health Insurance Service of Korea in 2020. However, multiple Korean versions of the EPDS are used for public health programs and research. This study aimed to summarize the use of this scale in Korea and evaluate the distribution of validities, depression scores, and prevalence of depression according to Korean versions of the EPDS.
Methods
Korean versions of the EPDS most frequently used in public health policies and programs were summarized through internet searches using snowball strategy. A systematic literature review was conducted to evaluate the prenatal and postnatal depression scores and prevalence of depression measured using different Korean versions of the scale.
Results
We identified four Korean versions of the EPDS that are commonly used in public health programs and research. Among them, published evidence regarding validity and reliability was available for two versions. A review of 19 papers that assessed prenatal and postnatal depression using these versions showed large heterogeneity in scores and the prevalence of depression.
Conclusion
When measuring prenatal and postnatal depression using the EPDS, characteristics of the scale must be considered when interpreting results. A standardized Korean version of the EPDS needs to be developed by comparing the validity and reliability of different Korean versions. A field manual for screening should also be developed and distributed.
서론
분만후우울증(산후우울증, postpartum depression)은 정신장애진단통계편람 5판(Diagnostic and Statistical Manual of Mental Disorder, DSM-5)에서 임신 중이나 출산 후 4주 내에 기분 증상이 발생하는 출산 전후 주요우울병삽화(major depressive episode)로 정의한다[1].
최근 수행된 체계적 문헌고찰 연구결과에 따르면 임신 중 우울증과 출산 후 우울증은 고소득 국가에서 각각 9.2%, 9.5%, 중·저소득 국가에서 각각 19.2%, 18.7%로 추정되었다[2]. 주요우울병의 유병률은 임신 중 3.1-4.9%, 출산 후 6개월 2.1-5.7%, 출산 후 7-12개월 1.0-3.9%로 알려져 있다[3]. 산후 우울감(baby blue)은 출산 후 1주에 나타나는 가볍고 일시적인 기분 저하로[4], 2018년 정부의 대규모 실태조사 결과 산모 중 50.3%가 산후 우울감을 경험하였다[5].
임신 중 우울증은 여성 자신의 물질 남용, 출산 후 우울과 불안[6,7], 출산 후 정신과 입원[8], 정신증[9]과 관련되었다. 또한 낮은 산전 진찰 횟수, 태아 신경 반응성 저하[10], 조산[11]의 위험요인으로 지적되었다. 출산 후 우울 증상은 의미 있는 타인과의 관계 유지 능력에 영향을 미치며 출산 전후 우울증은 임신 결과, 양육 스트레스와 태도, 아동 성장과 발달 등에 부정적인 영향을 미치는 것으로 알려져 있다[12-14].
임신한 모든 여성의 산전 진찰에서 정신병력과 더불어 현재의 정신건강에 대한 평가 수행이 국제적으로 권고되고 있다[15-17]. 출산 전후 우울증의 선별검사와 역학조사를 위해서 다양한 설문조사가 활용되고 있는데[18,19], 미국예방서비스특별전담조직(US Preventive Services Taskforce)은 임신 여성에 대한 우울증 선별검사로 에딘버러우울척도(Edinburgh Postnatal Depression Scale)를 제안한 바 있다[20]. 에딘버러우울척도는 Cox 등이 1987년 개발한 10문항으로 구성된 척도로, 정신장애진단통계편람 5판의 우울증 진단 영역 중 우울 기분, 관심과 즐거움의 감소, 수면의 변화, 무가치함이나 죄책감, 자살 생각을 다룬다[20]. 흔히 활용하는 우울 설문도구인 Patient Health Questionnaire-9, Beck Depression Inventory, Center for Epidemiologic Studies Depression Scale 등은 체중 변화, 피로 등 임신과 출산에 동반되는 증상을 포함하고 있다.
한국의 모성과 영유아의 생명과 건강을 보호할 목적으로 제정된 법률인 모자보건법은 2015년 12월 개정으로 제15조의 20을 신설하며 국가와 지자체의 산후조리 관련 실태조사 의무를 명시하였다. 2016년 12월 제10조의 5 분만전 및 분만후우울증 검사 등 지원을 신설하여 임신 전후 우울증의 조치에 대한 법적 기반이 마련되었다. 법·제도 조성과 더불어 2015년 분만후우울증 관리체계 구축방안 연구[21], 2017년 산후 정신건강 증진을 위한 지원 방안 연구[22], 2018년 산후조리실태조사[5] 등 일련의 국가적 실태조사와 정책 연구가 시행되었다. 2018년 처음 실시된 산후조리실태조사는 3년마다 실시되도록 규정되어 있으며, 분만후우울증에 관한 설문도구로 에딘버러우울척도를 사용하고 있다. 이어서 2020년 6월에는 건강보험 행위 급여·비급여 목록표 신경계 기능검사의 신설 척도에 에딘버러우울척도가 포함되면서 임상 현장에서 에딘버러우울척도의 사용이 건강보험 적용을 받게 되었다(보건복지부 고시 제2020-148호).
한국의 공공보건사업과 조사·연구에서 에딘버러우울척도는 다양한 한국어판이 활용되고 있다. 보건복지부가 운영하는 임신육아종합포털 아이사랑에서는 분만후우울증의 진단도구로 Kim 등[23]이 표준화한 에딘버러우울척도를 온라인으로 제공하고 있다. 한편 보건복지부 산전·조기 아동기 개입 프로그램인 생애 초기 건강관리 시범사업은 에딘버러 우울척도 원개발자의 책자에 포함된 한글 번역본을 활용하고 있다[24,25].
이 논문에서는 한국 중앙정부와 지역자치단체 단위 보건 정책과 사업에서 출산 전후 우울증 선별검사로 활용되고 있는 대표적 에딘버러우울척도의 종류와 내용을 파악하고, 각종 사업과 조사·연구의 활용 현황을 정리하였다. 또한 대표적 한국어판 에딘버러우울척도의 종류별 타당도와 출산 전후 여성의 우울 점수와 우울증 유병률을 요약함으로써 이 척도를 임상과 보건 실무에서 적용하고 해석할 때 기반이 될 수 있는 정보를 제공하고자 한다.
방법
연구자 회의를 통해 연구의 범위를 (1) 국내 한국어판 에딘버러우울척도 한국어판 에딘버러우울척도의 종류와 내용 파악, (2) 중앙정부와 지방자치단체 단위 보건 정책, 사업, 프로그램 및 조사·연구의 척도 활용 현황 조사, (3) 이 척도를 적용한 국내 출산 전후 우울 점수와 우울증 유병률 분포 요약으로 결정하였다.
한국어판 에딘버러우울척도의 종류와 활용을 조사하기 위해 인터넷 검색과 핵심 문헌을 통한 눈덩이 찾기 방법으로 법·제도, 중앙정부와 지방자치단체 단위 보건 정책, 사업, 서비스와 프로그램, 관련 문헌을 찾아 정리하였다. 설문 타당도 연구가 보고된 한국어판 척도를 우선하였으나, 정부의 보건사업에 활용되고 있는 경우 대표 한국어판으로 포함하였다.
대표 한국어판 척도를 적용하였을 때 출산 전후 우울 점수와 우울증 유병률 분포를 정리하기 위해 출판 문헌에 대한 체계적인 문헌 검색을 수행하였다. 국외 데이터베이스(MEDLINE, PubMed, EMBASE, Web of Science, PsychINFO)와 국내 데이터베이스(KoreaMed, KMBASE, KISS, RISS, NDSL, 국회도서관, 구글 학술검색[Google Scholar 한국어])에서 에딘버러우울척도(Edinburgh Postnatal Depression Scale, Edinburgh Depression Scale 등), 우울(depression, depressive disorder 등), 한국(Korea)을 조합하여 검색하였다. 검색은 2021년 1월 중에 시행하였다. 총 12개의 국내외 데이터베이스로부터 최초 취합된 연구논문의 수는 831편이었다. 수작업과 EndNote 서지프로그램을 활용하여 158건의 중복을 제거하였다. 이 중 논문의 유형이 초록, 학위논문, 학술대회 자료집 등 학술논문이 아닌 경우를 제외하고, 에딘버러우울척도에 관한 것이 아닌 것 등을 제외한 후 남은 논문의 수는 115편이었다. 이 중 지역사회 출산 전후 우울을 측정하였으며, 참여자가 100명 이상이면서 대표 한국어판 척도를 활용한 연구로 19편을 선정하였다. 김용구 판[23]을 적용한 연구가 12편, 한귀원 판[26]을 적용한 연구가 7편이었다(Figure 1).
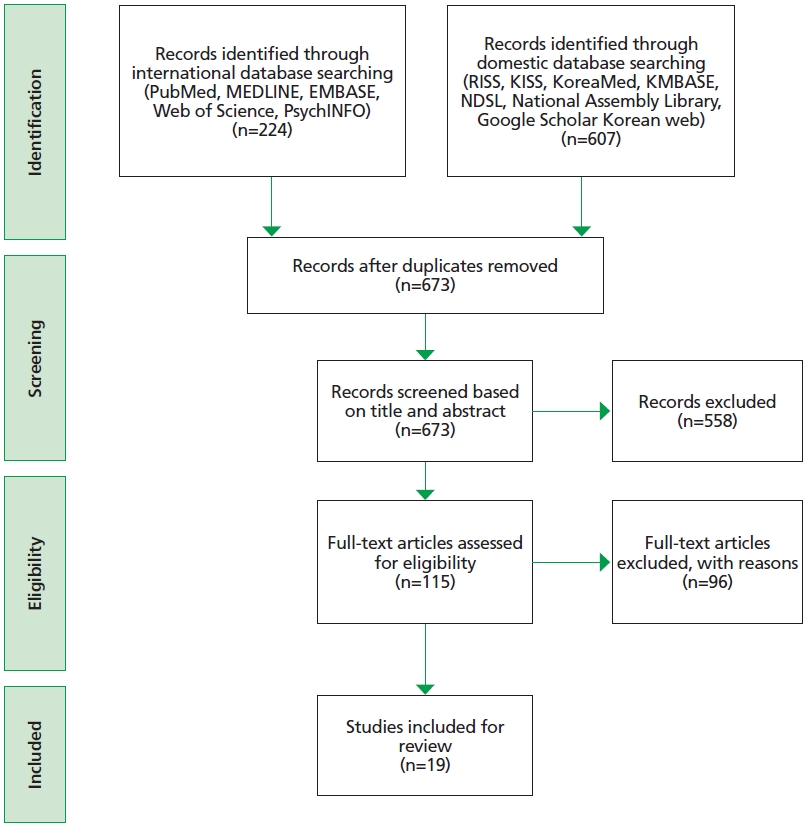
Flow chart for selecting the published papers.
결과
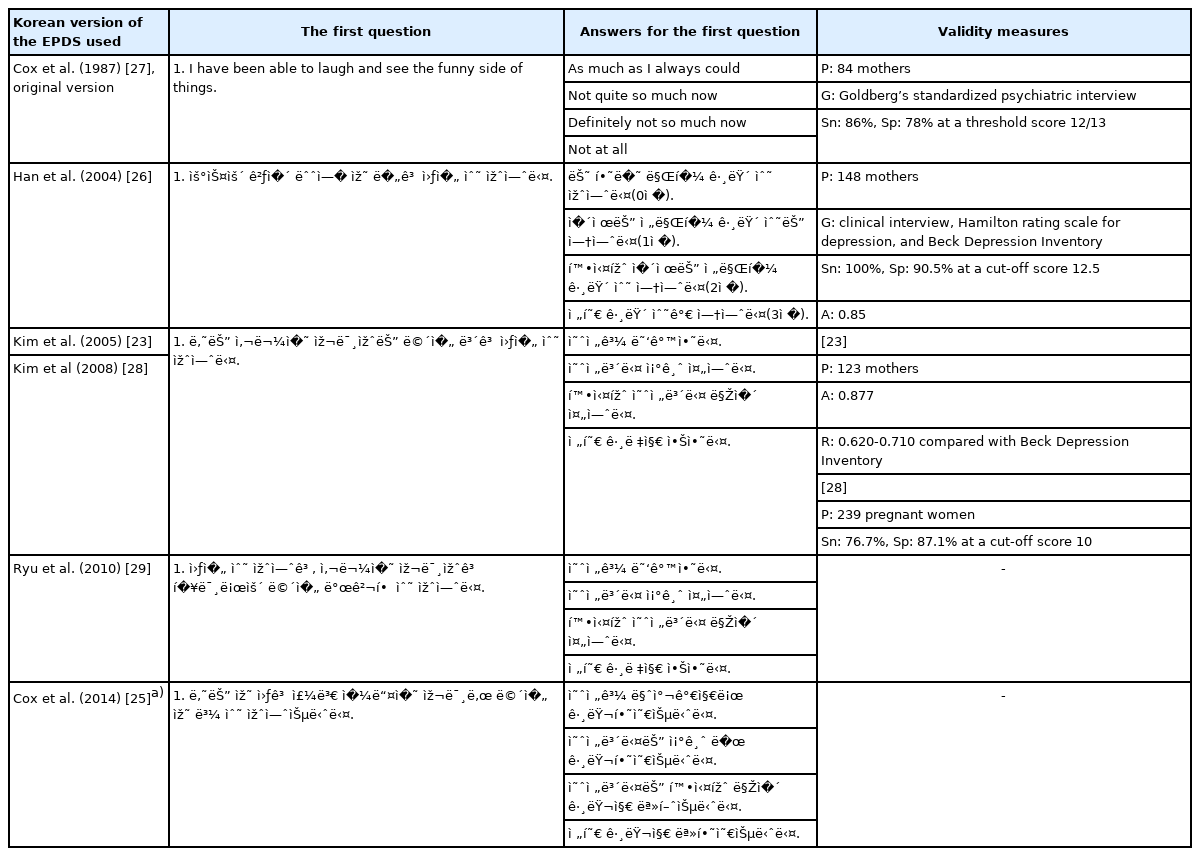
대표적인 한국어판 에딘버러우울척도의 종류는 Cox 등 원저자의 한국어판 번역과 2004년 한귀원 등, 2005년 김용구 등, 2010년 유애리 등의 판이 있었다(Table 1) [23,25-29]. 4개 한국어판의 내용과 원 에딘버러우울척도의 10개 문항을 비교한 내용은 부록으로 제시하였다(Suppl. 1) [23,25-27,29]. 4개 한국어판은 원문과 비교할 때 오역은 없다고 판단되나 표현과 용어에서 차이를 보였다. 1번 문항의 ‘I have been able to see the funny side of things’ 문장은 한귀원판의 경우 ‘우스운 것이 눈에 잘 띄었다’, 김용구 판은 ‘사물의 재미있는 면을 보았다’, 유애리 판은 ‘사물의 재미있고 흥미로운 면을 발견할 수 있었다’, Cox 등 원저자의 한국어판은 ‘주변 일들의 재미난 면을 잘 볼 수 있었다’로 모두 다르게 번역하였다. 4개 한국어판 중 타당도와 신뢰도를 보고한 한국어판은 김용구 판과 한귀원 판으로 총 2편이 있었다. 유애리 판의 경우, 분만후우울증의 위험요인을 확인할 목적으로 연구자들이 자체 번역하였으며, 타당도와 신뢰도에 대한 결과를 포함하고 있지 않았다. 또한, 에딘버러우울척도를 개발한 Cox 등의 원저자가 제시한 한국어판 척도는 다른 54개 언어의 번역판과 함께 소개되었지만, 타당도와 신뢰도를 제시하지 않았다.
The characteristics of biologics and biosimilars for the treatment of inflammatory bowel diseases
한국 중앙정부와 지방자치단체 단위에서 진행되는 보건 정책, 사업, 프로그램, 서비스와 조사·연구에 활용되는 에딘버러우울척도를 Table 2에 제시하였다[23,25,26,28-30]. 국민건강보험, 국가주도 사업, 지방정부 사업, 지자체 보건소 주도 사업, 국가주도 조사와 연구별로 정리하였다. 출산 전후 우울증을 예방, 선별검사, 완화하기 위해 다양한 종류의 한국어판 에딘버러우울척도가 활용되고 있었다.

Practical applications of different Korean versions of the EPDS
국민건강보험 급여목록에서는 에딘버러우울척도 중 특정한 한국어판을 지정하지 않았다. 정형화된 척도를 사용하여 검사를 시행한 뒤 결과를 진료기록부에 기재하면 보험 청구가 가능하다고 인정하고 있었다.
한편, 중앙정부와 지자체에서 수행하고 있는 사업들은 동일 운영주체 안에서도 프로그램이나 사업에 따라 서로 다른 한국어판 에딘버러우울척도를 사용하고 있었다. 예를 들어 보건복지부는 임산부와 영유아를 위한 정보를 안내하는 웹사이트인 임신육아종합포털 아이사랑과 정보 기록지인 모자보건수첩에 분만후우울증 자가평가를 위한 목적으로 김용구판 에딘버러우울척도를 소개하고 있었다. 하지만 보건복지부의 ‘생애 초기 건강관리 사업’에서는 간호사의 임산부 등록 평가 과정에서 Cox 등 원저자의 한국어판 에딘버러우울척도를 사용하고 있었고, 한국건강증진개발원의 지역사회 통합 건강증진사업 방문건강관리 매뉴얼에서는 면접조사표에 한귀원 판 척도를 사용하고 있었다. 한편 여러 지자체의 보건소 홈페이지에서 활용되는 에딘버러우울척도는 번역본의 출처를 밝히지 않았으며, 문항을 검색해도 출처를 확인할 수 없는 사례들이 있었고, Table 1의 대표 한국판 외 여정희 판[30]이 추가적으로 활용되고 있었다. 즉, 출산 전후의 여성들이 접근가능한 자료와 정보, 지역사회 건강관리 사업들에서 제각기 다른 버전의 에딘버러우울척도를 사용되고 있는 것을 확인할 수 있었다.
체계적 출판 문헌 검색 과정을 통해 19편의 문헌을 선정한 결과, 김용구 판이 적용된 경우가 12편, 한귀원 판이 적용된 경우는 7편이었다. 이 19편 문헌의 출산 전후 우울증 유병률과 척도의 평균값을 아래 Table 3에 요약하였다[23,26,28,31-49].
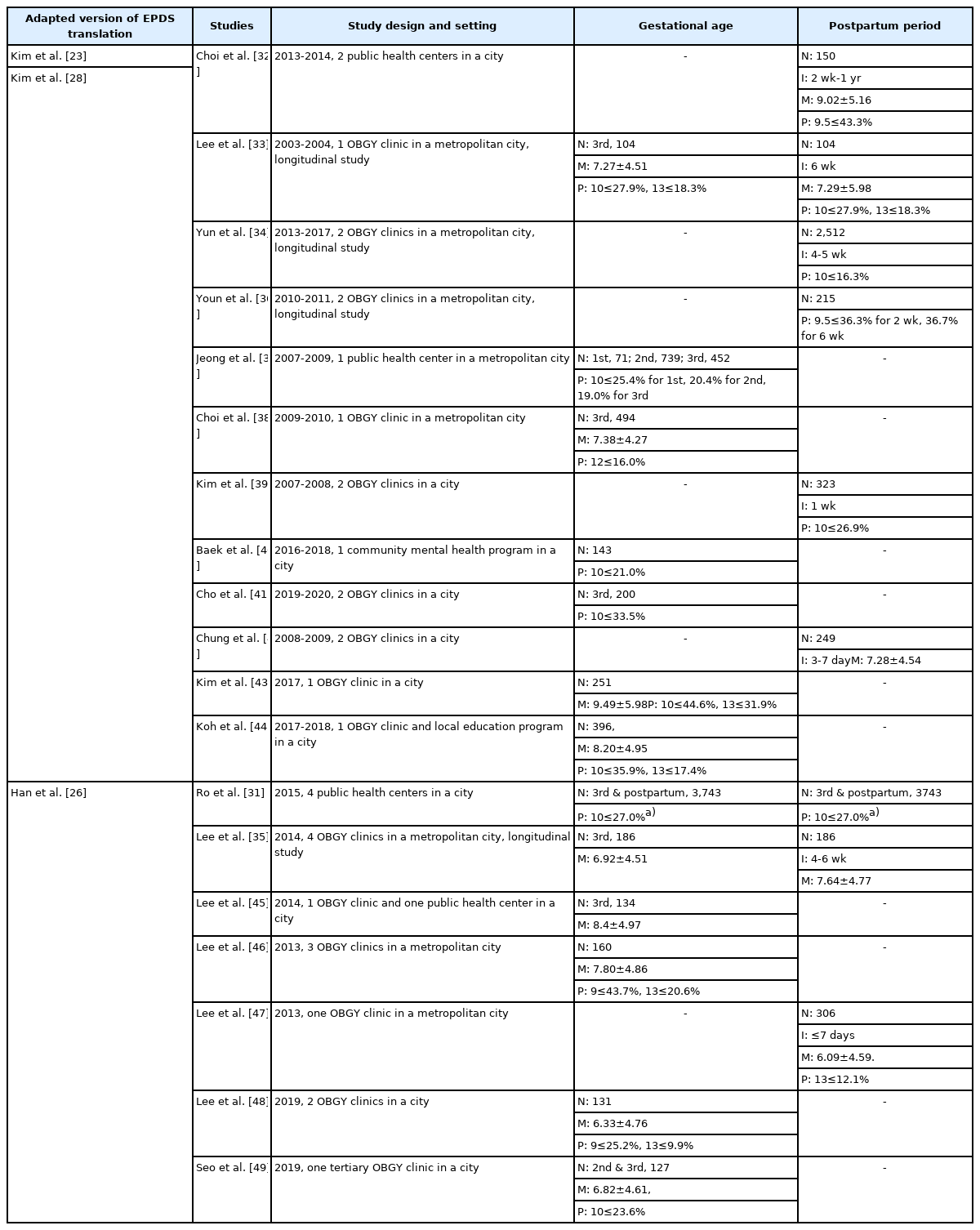
Perinatal depression prevalence and summary measures by two different Korean versions of the EPDS in Korea
연구 주제별로는 분만후우울증의 위험요인을 파악하는 연구가 11편으로 가장 많았고, 분만후우울증의 영향을 모성정체성, 태아애착행위 등 연구자의 관심 주제를 중심으로 확인하는 연구가 5편이었다. 이 외에 분만후우울증 측정 관련 연구가 2편 있었고, 지역사회에서의 분만후우울증 진단을 넘어 치료연계율을 파악한 연구가 1편[31] 있었다.
연구참여자는 지방자치단체 보건소, 정신보건센터 등 지역사회에서 모집한 경우와 산부인과 전문병원이나 대학병원 산부인과에서 모집하는 경로로 구분되었다. 참여자 거주 지역은 특별시와 광역시, 시 단위 지역사회로써, 농촌 지역은 없었고 전국 단위나 여러 지역사회를 포함한 연구는 없었다. 임신 시기를 1-2기와 3기, 산후로 나누었을 때, 각 시기별로 표본을 구분하여 조사를 실시하고 에딘버러우울척도 점수와 우울증 유병률을 제시한 연구도 제한적이었다. 시기별로는 임신 3기를 포함한 연구가 13편으로 가장 많았고, 산후를 포함한 연구가 9편, 임신 1기 또는 2기를 포함한 연구가 7편으로 가장 적었다. 산후 기간의 범위는 최소 7일 이내에서 최대 1년까지 존재하였지만, 산후의 시기를 6개월[31], 또는 1년까지[32] 넓게 확인한 연구의 수가 상대적으로 적었다. 즉, 에딘버러우울척도를 활용해 출산 전후 우울증을 측정한 연구 중에는 임신 초기와 출산 후의 기간을 폭넓게 포괄하는 연구가 많지 않은 것으로 나타났다.
에딘버러우울척도의 절단점은 10점을 적용한 연구가 11편(57.9%)으로 가장 많았고, 5편에서 13점을 적용하였다. 출산 전후 시기에 따른 종단연구는 4편이었으나, 대사물질의 변화[33], 수면 박탈[34]과 같은 다른 변수를 초점에 두거나 분만후우울증 관련 요인 분석을 주제로 하여[35], 출산 전후 시기에 따라 점수와 유병률의 변화를 추적한 연구는 1편[36]이었다. 이 연구에서 에딘버러우울척도 10점 이상은 출산 2주 36.3%, 출산 6주 36.7%로 보고되었다[36].
한귀원 판을 적용하여 1개 경기도 시 단위 지역에서 보건소를 통해 출산 전후 3,743명 여성을 선별검사한 연구는 10점 이상 위험군을 27.0%로 보고하였다[31]. 이 연구는 우울 선별검사 후 의뢰를 연구주제로 하였기 때문에 출산 전후 시기에 따라 10점 이상 위험군의 유병률을 별도로 보고하지 않았으나 연구대상의 84.7%가 임신 여성이었다. 서울특별시 1개 보건소에서 1,262명의 임신 여성에게 김용구 판을 적용한 연구에서 10점 이상은 20.2%였으며[37], 제시된 임신 시기별 분포를 통해 산출한 임신 시기별 10점 이상 유병률은 1-3기 각각 25.4%, 20.4%, 19%였다. 서울특별시 산부인과 전문병원 2곳에서 출산 4-5주 2,512명을 대상으로 김용구 판을 적용한 연구는 10점 이상 우울 증상 유병률을 16.3%로 보고하였다[34]. 김용구 판을 적용하여 서울특별시 1개 대학병원 산부인과에 산전 진찰을 목적으로 내원한 494명의 임신 3기 여성을 대상으로 한 연구에서 12점 이상은 16.0%로 조사되었다[38]. 이 4편을 제외한 연구는 연구대상자수가 모두 400명 미만이었으며, 200명 이하의 연구 대상자를 조사한 연구가 9편(47.4%)이었다. 동일한 한국어판을 적용한 연구 안에서도 평균값과 유병률의 범위가 비교적 넓게 보고되었다.
고찰
1994-2012년 동안 적용된 정신장애진단통계편람 4판은 주요우울장애의 임신 관련 시기의 특정자(specifier)로, 출산 후 4주라는 산후시기를 적용하였다. 임상과 연구의 측면에서 산후시기를 출산 전후 시기로 확장하여야 할 필요성이 제기되었고[50], 2013년부터 적용된 정신장애진단통계편람 5판에서 임신 중과 출산 후 4주로 시기를 정의하게 되었다. 임신 중 우울과 불안은 출산 후 우울의 위험을 증가시키며[6], 출산 후 우울증의 약 50%는 임신 시기에 발생한다[50]. 외국의 대규모 코호트 연구에서 임신 중 우울증이 출산 후 우울보다 더 흔하였으며[51], 임신 중 우울 증상이 과거에 비해 근래 더 증가하였다는 보고도 있다[52]. 분만후우울증이라는 용어는 질병 정의와 다르게 질병 발생 시기를 출산 후로 협소하게 이해하게 만들어 오해를 유발할 가능성이 있다. 현재 한국 보건복지부가 운영하는 임신과 육아에 대한 대국민 정보채널인 아이사랑에서도 분만후우울증을 출산 직후 나타나는 산모의 우울증으로 정의하고 있는 형편이다. 따라서 임신 중(during pregnancy, antenatal, antepartum) 우울증과 출산 후(following delivery, postnatal, postpartum) 우울을 모두 통칭하는 출산 전후(perinatal, peripartum) 우울증으로 용어를 사용할 필요가 있다.
국제적으로 산전 진찰과 산후관리에서 우울 선별검사가 권고되며[15-17], 미국예방서비스특별전담조직은 임신 여성에 대한 우울증 선별검사로 에딘버러우울척도를 제안하였다[20]. 에딘버러우울척도는 1987년 Cox 등이 개발한 이후 출산 전후 우울증의 선별검사 도구로 인정받고 있으며, 다양한 연구활동에 활용되고 있다. 최근 체계적 문헌고찰 연구에 의하면 10점, 11점, 13점 절단점에서 출산 전후 우울증의 민감도는 각각 85%, 81%, 66%였으며, 특이도는 84%, 88%, 95%로 조사되었고, 임신 여성과 출산 후 시기에 따른 차이는 없었다[53].
한국에서도 2000년대 중반 이후 분만후우울증 척도로 다양한 연구자에 의해 한국어판이 소개되어 활용되었다. 여러 보건사업과 조사·연구에 활용되는 한국어판은 4종으로 추려졌다. 이 중 타당도와 신뢰도 연구 근거가 출판된 것은 김용구 판과 한귀원 판이었다. 한국 중앙정부와 지방자치단체 단위 보건 정책, 사업, 프로그램, 서비스와 조사·연구에 활용되는 에딘버러우울척도는 다양하였으나 출처를 밝히지 않은 척도가 많았으며, 앞서 선별한 4종이 빈번하게 활용되고 있었다. 2020년 6월 한국 건강보험 행위 급여·비급여 목록표 신경계 기능검사의 신설 척도에 ‘에딘버그산후우울척도’란 명칭으로 에딘버러우울척도가 포함되면서 임상 현장에서의 사용이 건강보험 적용을 받게 되었는데, 건강보험 2021년 점수당단가(환산지수)를 반영할 경우 3,790-4,290원에 해당한다. 국민건강보험 신경계 기능검사에서 에딘버러우울척도의 구체적인 한국어판의 종류는 지정되지 않았다.
체계적 문헌 검색을 통해 에딘버러우울척도를 한국 출산 전후 여성에게 적용한 출판 문헌을 검색하였다. 김용구 판과 한귀원 판을 적용한 19편의 문헌을 선정하였는데, 지역사회와 임상환경, 연구대상자 거주 지역사회, 임신 시기와 출산 전후 시기에서 연구 간 이질성이 컸고, 척도의 평균과 유병률 결과값의 범위가 컸다. 이러한 표본의 이질성으로 인해 메타분석을 통한 총합 추정치(pooled estimator)를 산출하기는 어려웠다. 에딘버러우울척도 10점 이상의 유병률은 임신 여성에서 19.0-44.6%였으며, 출산 후 6주까지 10점 이상 유병률은 12.1-36.7%의 범위를 보였다.
출산 전후 우울증의 조기 발견과 개입을 위해서는 척도 활용을 통한 진단뿐 아니라 진단 이후 적절한 정신건강 서비스를 의뢰 및 제공하여 연계율을 제고하려는 노력이 필요하다. 하지만 해외에서도 연계율(referral completion rates)은 체계적으로 추적되지 못하고 있는 실정이며[54], 이 연구에서 선정한 논문 중 의뢰와 연계를 다룬 논문은 한 편뿐이었다. Ro 등[31]은 에딘버러우울척도를 활용해서 지역사회에서의 분만후우울증 유병률을 파악하고 분만후우울증이 있는 것으로 확인된 산모들을 대상으로 인근 병의원 연계를 권유한 뒤 치료연계율을 파악했다. 해당 논문에서 파악된 고위험 산모 99명 중 치료가 연계된 산모는 총 8명(8.1%)이었다.
이 연구는 조작적 정의(operational definition) 방법으로 검색한 출판 문헌과 온라인 접근이 가능한 사업만을 포함하였으며 학위논문과 연구결과가 발표되지 않은 현재 진행 중인 프로젝트는 배제하였다. 그러나 한국에서 출산 전후 우울증에 에딘버러우울척도를 적용하고 해석하고자 할 때, 이 연구에서 제시한 한국어판과 원문의 차이, 타당도 지표, 유병률의 수준은 중요한 정보가 될 것이다.
한국에 대표적으로 활용되는 4종의 한국어판을 적용한 결과를 비교하기 위해서, 한국어판 유형 간의 신뢰도 연구가 추가적으로 요구된다. 또한 에딘버러우울척도를 개발한 Cox 등이 제공하는 한국어판[25]의 타당도와 신뢰도에 대한 확립도 긴요하다.
한국에서는 출산 전후 여성의 우울증과 아동 건강에 대한 관심이 커지고 있기 때문에 에딘버러우울척도의 활용에 있어 척도의 도입만이 아니라 출산 전후 우울증에 대한 이해와 척도의 활용법에 대한 가이드도 필요하다. Cox 등은 출산 전후 정신건강: 에딘버러우울척도 사용 매뉴얼(Perinatal Mental Health: The Edinburgh Postnatal Depression Scale Manual)을 발간하여 일차의료와 이차의료에서 척도의 활용을 위한 정보를 제공하고 있는데, 이 매뉴얼에 대한 한글화와 현장 적용가능성을 고려한 배포도 추후 고려되어야 할 것이다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HI19C0481, HC19C0048).
Supplementary Materials
Supplementary materials are available from https://doi.org/10.5124/jkma.2021.64.10.699.
Comparison of ten items among different Korean versions of the Edinburgh Postnatal Depression Scale
References
Peer Reviewers’ Commentary
이 논문은 20% 정도의 유병률에도 불구하고 그 중요성이 간과되고 있는 임신 중 또는 분만후우울증(산후우울증)의 선별 도구인 에딘버러우울척도 한국어 판의 신뢰도와 타당도 및 그 활용 현황을 정리한 논문이다. 주산기우울증은 산모와 영유아의 건강에 심각한 결과를 초래할 수 있는 질환으로 이를 잘 관리하는 것이 공중보건의 주요 과제 중 하나이다. 최근 수년 전부터 정부도 그 중요성을 인식하여 관계 법령의 개정을 통해 주산기우울증의 치료관리체계를 구축해 오고 있다. 에딘버러우울척도는 주산기우울증의 치료관리에 핵심적 역할을 하는 선별도구인 반면, 국내에는 다양한 번역본이 있어 지자체별 및 사업별로 통일성 있게 사용되지 못하고 있어 그 활용 현황을 조사한 이 논문은 공중보건학적으로 중요한 의미를 갖는다. 이 논문은 산후우울증 연구에 있어서 사용해야 할 에딘버러우울척도의 공인된 한국어판과 현장 지침 개발의 필요성을 잘 제시하고 있는 좋은 논문으로 판단된다.
[정리: 편집위원회]