서론
심부전이란 심장의 구조적 혹은 기능적 이상으로 말초 조직에 필요한 만큼의 혈류를 전달하지 못하는 상태를 나타내는 임상 증후군으로 특징적인 징후(경정맥압 상승, 폐수포음 등)와 증상(호흡곤란, 부종, 피로감 등)이 동반된다[1]. 심부전의 유병률은 증가하고 있으며 사망률이 높은 중증 질환이고, 사회 경제적 비용이 높기 때문에 질병에 대한 적절한 이해와 관리가 매우 중요하다[2]. 현재 심부전은 심장 초음파상의 좌심실 박출률(left ventricular ejection fraction, LVEF)을 기준으로 분류한다. 박출률이 50% 이상 보존되어 있는 경우 박출률 보존 심부전(heart failure with preserved ejection fraction, HFpEF)이라고 하며, 박출률이 40% 미만인 경우 박출률 감소 심부전(heart failure with reduced ejection fraction)으로 정의한다[1,3-5]. 박출률이 41-49%인 경우 박출률 중간 범위 심부전 혹은 박출률 경한 감소 심부전(heart failure with mid-range ejection fraction or heart failure with mildly reduced ejection fraction)으로 정의하는데, 이러한 cut-off가 적절한지, 성별에 따른 차이를 두어야 하는 것은 아닌지 등에 대해서는 아직 논란이 있다. 참고로 유럽심장영상학회에서는 박출률의 정상 범위 기준을 남성 52%, 여성 54%로 정의한 바 있다[6].
HFpEF의 병태생리
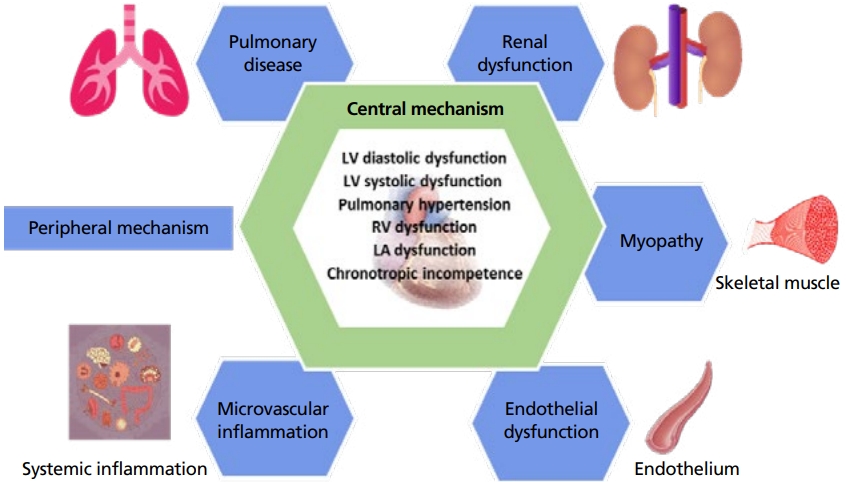
이완기능 장애(diastolic dysfunction)가 HFpEF 병태생리의 근간을 이루지만, 이완기능 장애 이외에도 다른 심장 관련 병태생리와 심장 이외의 전신적인 병태생리도 HFpEF 발생에 중요한 역할을 하는 것으로 알려져 있다[9-11]. HFpEF는 매우 다양한 원인에 의해 다양한 임상 양상(phenotype)을 보이기 때문에 각각의 개별적인 치료가 우선적으로 필요할 수 있다(예: 고혈압, 관상 동맥질환, 아밀로이드증, 심방세동, 판막질환) [1,9,12-14]. HFpEF의 병태생리에 대한 모식도를 Figure 1에 표현하였다[11]. 박출률 감소 심부전과 비교했을 때 HFpEF 환자는 대체로 고령이거나 여성인 경우가 많고, 심방세동, 만성 신부전, 심장 이외의 전신적인 질환이 동반되는 경우가 흔하다[15-18].
1. 이완기능 장애
좌심실충만압(Left ventricular filling pressure) 상승은 이완기능 장애를 나타내는 중요한 지표이다. 좌심실이완기말압), 평균이완기압, 평균좌심방압, left ventricular pre-A pressure, 평균폐모세혈관쐐기압 등이 모두 좌심실충만압을 표현하는 데 사용된다. 최근 연구에 따르면, 평균폐모세혈관 쐐기압이나 left ventricular pre-A pressure가 12 mmHg 이상이거나, 좌심실이완기말압이 16 mmHg 이상일 경우 비정상적인 좌심실충만압으로 판단할 수 있다[19]. 좌심실이완 기말압은 좌심방 수축 이후, 심실 수축 직전의 값으로, 보통 평균 좌심방압보다 높지만, 전부하를 잘 반영할 수 있다. 따라서 좌심실이완기말압은 좌심실전부하와 좌심실 이완능력을 함께 보여주는 값이라고 할 수 있고, 정상좌심방압이면서, 좌심실탄성이 떨어진 상태에서도 상승될 수 있다. 이에 반해 평균폐모세혈관쐐기압은 좌심방과 좌심실을 통해 폐순환에 가해진 압력을 모두 반영하는 값이다. 폐동맥고혈압과 연관된 HFpEF의 평가에서는 심방과 심실압의 총체와 폐동맥의 역동적인 값을 측정하기 위해 폐모세혈관쐐기압을 측정한다.
HFpEF는 다양한 원인 질환에 따라 다양한 임상 양상을 갖지만, 분자세포학적으로는 심근세포의 강성도와 섬유화 증가가 심부전 발병에 중요한 역할을 하는 것으로 알려져 있다[20]. 가장 기본단위인 근섬유분절의 운동 결함, cyclic guanosine monophosphate (GMP)-protein kinase G (PKG) 신호의 결함, 미세혈관의 허혈, 미토콘드리아의 대사장애 등이 동반된다[20,21]. Titin과 actin의 상호작용이 심근세포의 강성도를 결정하는 중요한 요소인데, 일종의 용수철과 같은 역할을 하는 titin이 저인산화(hypophosphorylation)가 될 경우 cyclic GMP-PKG activity가 감소되어 강성도가 높아지면서 HFpEF가 초래될 수 있다[9,22].
2. 이완기능 장애 이외의 심장기능 이상
HFpEF 환자에서 이완기능 장애 이외에도 다양한 심장 기능 장애가 나타나는데 좌심실 수축기능 장애, 폐동맥 고혈압, 우심실기능 부전, 좌심방기능 장애, 심박수 변동부전(chronotropic incompetence) 등이 포함된다.
2) 폐동맥고혈압과 우심실기능 부전
폐동맥고혈압은 심부전 환자에서 호흡곤란이 발생하는 가장 중요한 기전이다. 이완기능 장애, 수축기능 장애, 부정맥, 판막질환 등 다양한 기전으로 인해 좌심실충만압이 증가하게 되면 폐동맥고혈압이 초래될 수 있다. 심부전 환자의 약 60% 이상에서 폐동맥고혈압이 동반되는 것으로 알려져 있으며, 폐동맥고혈압이 동반되는 경우 LVEF 수치와 관계없이 예후가 좋지 않으며, 특히 총 사망률과도 연관성이 높다[12,20,24]. 좌심실기능 저하로 발생한 폐동맥고혈압은 우심도자술에서 폐동맥압은 25 mmHg 이상이면서 동시에 평균폐모세혈관쐐기압도 15 mmHg 이상으로 나타난다. 높은 평균폐모세혈관쐐기압이 지속되면 precapillary 혈관에서도 병리적 리모델링이 일어나며, 결국 isolated post-capillary PH로부터 combined pre-and post-capillary PH (Cpc-PH) 형태의 폐동맥고혈압이 발생하게 된다[25]. HFpEF의 경우 박출률 감소 심부전보다 좌심방이 더 일찍 뻣뻣해 지고, 기능의 저하가 더 일찍 발현되고, 심방세동과 같은 부정맥에 취약해지고, 세포분자환경에서 염증에 더 많이 노출되는 환경이 조성되어 Cpc-PH-HFpEF가 발생한다고 알려져 있으며, HFpEF 환자에서 Cpc-PH의 빈도가 더 높은 것으로 알려져 있다[25,26]. 우심실기능 부전은 HFpEF에서 흔히 발생할 수 있고, 폐동맥고혈압이 지속되면, 삼첨판 역류증과 우심실기능부전이 발생하게 된다[12,20]. HFpEF 환자에서 우심실기능부전이 동반될 경우 예후가 불량하다.
3. HFpEF의 전신적인 병태생리
1) 내피세포기능 저하
HFpEF에서 심장기능의 병태생리와 심장 이외의 전신적인 병태생리를 포괄하는 중요한 개념이 전신적인 미세혈관의 염증 반응 및 내피세포기능 저하이다. 노화, 비만, 내당능 장애, 고혈압 등에 의해 전신적인 혈관의 내피세포기능 저하가 HFpEF의 발병과 관련되어 있는 것이 잘 알려져 있고 이는 산화질소(nitric oxide) 감소에 따른 GMP 감소, PKG 신호 감소의 기전으로 발생한다. 특히 대동맥뿐만 아니라 말초 혈관의 경직도가 증가하면서 후 부하가 증가하게 되면 심장의 재형성이나 섬유화, 이완기능 장애, 폐동맥 고혈압 등이 더욱 악화된다[30].
3) 폐기능 장애
HFpEF 환자에서 좌심실충만압이 지속적으로 상승하면, 폐 질환도 흔하게 동반되는데, 좌심방압증가와 함께 폐혈관 저항이 증가하고, 폐정맥 내피층의 비대와 섬유화가 발생하면 폐의 산소 교환 능력이 저하되고 이는 운동능력 저하와 연관된다. 폐혈관의 재형성이 진행되면 우심실기능부전이 발생하고 이는 심박출량 감소로 이어진다.
4) 신장기능 장애
신장기능 장애는 심장기능 장애와 양방향에서 이해해야 한다. 신장기능 저하가 HFpEF의 발생에 영향을 주지만, HFpEF 자체에 의해서도 전신적인 정맥 울혈이 발생하고, 이에 따른 신장기능 저하가 발생하기 때문이다. 전신 혈압은 낮지만 신장 정맥압이 상승하면 신장으로의 혈류 공급 장애가 발생한다. 신장 내 울혈과 신장 내 압력 상승은 결국 중심 정맥압의 상승과 연관되고, 우심실기능 저하에 기여하게 된다. 심장과 신장의 이러한 양방향적인 관계는 아직 완전히 이해되지 않았지만, HFpEF의 위험성이 있는 환자 중 어떤 환자에서는 심부전의 증상과 징후가 발생하지만 다른 환자에서는 임상적인 증상을 보이지 않는지에 대한 실마리를 신장기능 이상에서 찾을 수 도 있다[20].
HFpEF의 진단
HFpEF에 대하여 다양한 임상연구에서 서로 다른 진단적 기준을 제시해 왔다. 최근에는 진단 보조를 위해 H₂FPEF와 HFA-PEFF 라는 두 가지 점수에[24,34], 기반을 둔 알고리즘이 제시된 바 있고, 어떤 점수체계를 따르냐에 따라 HFpEF로 분류되기도 하고, 추가적인 검사가 필요한 경우도 있다[35,36]. 변수들 중에서 좌심방 크기(left atrial volume index)가 32 mL/m²를 넘는 경우, 조기 충만 최대 혈류 속도(mitral E velocity)가 90 cm/s 미만인 경우, 조기 충만 심근 속도(septal e’ velocity)가 9 cm/s 미만인 경우, 조기 충만 승모판 유입 혈류 속도와 조직 속도의 비율(E/e’)이 9를 넘는 경우 심혈관계 사망률이 유의하게 증가하는 임계점으로 알려져 있다. 간략하게는 다음과 같은 세 가지 조건을 모두 만족해야 HFpEF로 정의할 수 있다. (1) 심부전의 증상과 징후, (2) LVEF ≥50%, (3) 심장질환의 구조적 그리고/혹은 기능적 장애와 나트륨배설펩타이드(natriuretic peptide) 상승을 포함해서 좌심실 이완기능 장애 및 좌심실충만압 상승과 일치되는 객관적 증거[24,37].
참고로 이전에 심박출률 감소 심부전 환자였는데 치료를 받는 중에 박출률이 50% 이상으로 호전되었을 때 이를 HFpEF라기 보다는 recovered HF, HF with improved LVEF로 간주하는 것이 바람직하다. 박출률 감소 심부전에 준해서 약물치료를 계속하는 것이 추천되는데, 수축기능 회복을 보인 환자에서 얼마 동안 약물치료를 지속해야 하는지에 대해서는 아직 논란이 있다. 심방세동이 동반된 경우, left atrial volume index의 기준을 40 mL/m²로 한다. 운동부하 심초음파에서는 E/e’ ratio ≥15, 삼첨판 역류 최고 혈류 속도 >3.4 m/s로 기준한다[37].
안정 시 심장 초음파검사 결과와 혈액검사상의 B-type natriuretic peptide (BNP), N-terminal pro-BNP의 결과가 불일치할 때, HFpEF의 확실한 진단을 위해서 추가 검사로 호흡곤란의 원인을 감별하고, 운동능력의 감소를 확인하기 위해 cardiopulmonary exercise testing과 운동부하검사, 그리고 침습적 혈역동학 운동검사를 고려할 수 있다. 확진을 위해서는 침습적으로 폐모세혈관쐐기압력을 측정하여, 폐모세혈관쐐기압 ≥15 mmHg(안정 시) 혹은 ≥25 mmHg (운동 시) 혹은 이완기말확장압 ≥16 mmHg인 경우 HFpEF로 진단할 수 있다[24,37].
HFpEF의 치료
현재 HFpEF의 치료는 질병의 경과를 호전시키는 것에 대한 권고사항이 충분하지 않은 만큼, 치료의 목적은 증상의 완화에 있다. 울혈로 인한 증상에서는 이뇨제를 적절히 사용해야 하며 고리 이뇨제(loop diuretics)가 우선 추천되고, thiazide 또한 고려될 수 있다. 비만한 체구에서는 체중감량과 운동 치료가 증상의 개선과 운동능력 개선에 도움을 준다.
약물치료의 경우 일부 특정 유형의 HFpEF 환자에서 예후 개선 효과를 보여준 소규모 연구도 있었으나, 많은 수의 HFpEF 환자를 대상으로 한 perindopril in elderly people with chronic heart failure (PEP-CHF [perindopril)]) [38], CHARM-Preserved (candesartan) [39], I-PRESERVE (irbesartan) [40], TOPCAT (spironolactone) [41], DIG-Preserved (digoxin) [42], 그리고 PARAGON-HF (sacubitril/valsartan) [43] 등의 대부분의 무작위 임상연구에서 유의한 예후 개선 효과를 보인 치료가 없었다. 하지만 candesartan이나 spironolactone, sacubitril/valsartan의 경우 심부전 악화에 의한 입원을 감소시키는 경향은 확인할 수 있었다. 이외에 베타차단제와 Nitrioxide 제제에 관한 연구들은 운동능력 향상이나 삶의 질 향상에 통계적으로 유의한 개선 효과는 보여주지 못했다(Nitrate’s Effect on Activity Tolerance in [NEAT]-HFpEF [44], INDIE-HFpEF [45]).
미국 식품의약국에서는 최근 안지오텐신수용체-네프릴리신억제제와 염류코티코이드대항제의 사용을 정상보다 낮은 심박출 심부전 환자에서 사용을 허가하였다. 이는 박출률 경한 감소 심부전과 HFpEF를 아우르는 권고사항이다. 안지오텐신수용체-네프릴리신억제제에 관하여는 PARAGON-HF의 하위그룹 분석의 결과에서 EF<57%인 환자에서 심부전 입원율이 감소한 점과 또한 PARADIGM-HF와 PARAGON-HF의 메타분석에서 정상보다 낮은 심박출 심부전 환자에서 심혈관계 사망과 심부전 입원율의 감소의 결과에 근거한다. 염류코티코이드억제제에 관하여는 TOPCAT 연구의 하위그룹 분석에서 일차 종말점인 심혈관계사망과 심부전 악화에 의한 입원율의 상당한 감소효과를 보여주었다.
한편, 최근 HFpEF 환자를 대상으로 한 EMPEROR-Preserved 연구결과가 발표되었는데 EF >40%인 New York Heart Association class II, III, 혹은 IV에 해당하는 5,988명의 HFpEF 환자를 대상으로 기존의 일반적인 치료에 더하여 empagliflozin 10 mg를 추가하였을 때 일차 종말점인 심혈관계 사망과 심부전 악화에 의한 입원을 유의하게 감소시키는 것으로 확인되었다. EMPEROR-Preserved 연구는 현재까지 시행된 HFpEF 환자를 대상으로 한 연구 중 가장 큰 규모로 심혈관계 사망에서는 큰 차이가 없었지만, 심부전에 의한 총 입원 횟수를 매우 유의하게 감소시켰고, 당뇨병 동반 여부와 관계없이 일관되게 예후를 개선시키는 것으로 확인되었다[46,47]. 그동안 HFpEF 환자를 대상으로 진행된 다양한 임상연구에서 명확한 예후 개선 효과를 입증한 약제가 없었기 때문에 HFpEF의 치료는 혈압 조절이나 심박수 조절, 이뇨제를 통한 증상 조절, 동반 질환에 대한 치료 등으로 상당히 제한되어 있었다. 특히 HFpEF 환자는 매우 다양한 임상 양상을 보이기 때문에 한 가지 약제로 모든 스펙트럼의 환자의 예후를 일관되게 개선시키기 어렵다는 의견이 많았음에도 불구하고, empagliflozin이 본 연구를 통하여 예후 개선 효과를 뚜렷이 보여줌으로써 향후 HFpEF의 병태생리에 대한 새로운 이해와 추가적인 치료제 개발에도 중요한 계기를 마련하였다. 또 다른 sodium-glucose cotransporter 2 억제제에 대한 연구로 DELIVER study가 있고, EF >40% 이상의 환자에게서 dapagliflozin이 심혈관계 원인에 의한 사망과 심부전의 악화를 감소시킬 수 있을지에 대한 연구가 진행 중이며 2022년 상반기에 결과가 발표될 예정이다.
HFpEF 환자에 대한 기구 치료로 심방 단락(interatrial shunts)이 비교적 활발히 연구되고 있는데 이는 좌심방과 우심방 사이의 혈액을 원활히 순환시켜 잠재적으로 폐울혈을 완화시키는 치료이다. 이외에도 심박수 변동부전에 대한 심박수 적응 조율 장치(rate adaptive pacing)나 심장 재동기화 치료(cardiac resynchronization therapy), 심근 수축력 조절 장치(cardiac contractility modulation)나 좌심방 조율 장치 등이 연구되고 있다.
결론
HFpEF는 심혈관계 분야에서 가장 중요한 미해결 질환으로서 다양한 표현형에 대한 구체적인 병태생리 기전을 이해하려는 노력이 필요하다. 최근 안지오텐신수용체-네프릴리신억제제와 염류코티코이드대항제가 HFpEF 환자의 약물치료로 허가되었고, EMPEROR-Preserved 연구를 통하여 empagliflozin이 당뇨병 동반여부와 무관하게 예후를 개선시키는 것으로 확인되었다. HFpEF 환자에서 기저 위험요인과 동반 질환을 적절히 평가하여 치료하고 예방하는 것이 중요하다[43].